There is something special about Laguna Honda hospital in San Francisco, and Dr. Victoria Sweet can’t quite put her finger on it. At the beginning of her tenure at the sprawling institution, a fellow physician tells her that Laguna Honda is a gift. “You’ll see,” he says cryptically, before walking off down the corridor.
Sweet’s book is an exploration of questions that arose early in her career, standing over an autopsy table, plagued by unanswered questions about the essence of life. What happens to it? Where did that thing go that gave this body such animation and purpose?
God’s Hotel is itself an autopsy into the life and times of a hospital that represents a passing era of charity, miracles, and slow medicine. Sweet undertakes an examination of soon-to-be-decommissioned Laguna Honda—one of the United States’ last almshouses—with a view of the whole modern medical system in flux. She seeks the essence that gave the hospital such efficacy and spirit. An autopsy is, after all, latin for “seeing for oneself” and this examination allows us to peek inside the system, to understand the ways we deliver care to the sick (particularly the sick poor), and just as importantly, why we do so.
Hildegard and the Hospital
Laguna Honda functions on three principles: hospitality, community, and charity. These principles are closely intertwined and depend on each other. Sweet delves into the roots of our modern vernacular to understand the purpose and interactions of community (communio), hospital (hospitalis), life (anime), and spirit (spiritus). The term hospital originated in hospitalitas, or hospes: to care for the traveller, stranger, or pilgrim, with the understanding that in another circumstance, the host might need the same care. The community was central to hospitality because it was a collective community-driven exchange, an unspoken agreement.
Sweet carries us into a sweeping history of medicine, beginning in the middle ages with a twelfth century Benedictine nun, theologian, mystic, and physician named Hildegard. Stepping back in time from the reductive medicine of the modern west, Sweet experiments with Hildegard’s ideas in her own practice, using her simple, and not-so-outlandish strategies for diagnosis and treatment. Hildegard married theology and faith with medicine. She knew that true healing meant gaining wholeness of both the body and the spirit, by being attuned to the environment inhabited by the patient, and slowly restoring function to the ill person. In studying Hildegard, Sweet’s explorations quickly turn to the spiritual, and she runs straight into God in her search for what’s missing.
In most western settings, medicine is a commodity and its specialized practitioners “sell their wares” in a systematized, highly regulated trade. Healthcare has been absorbed into the machinations of the free market. Patients are client-consumers, hospitals are providers, and the system is monitored for efficiency or inefficiency based on dollars spent, saved, and wasted.
Sweet finds, however, that seemingly inefficient, old-fashioned practices at Laguna Honda actually function with their own incalculable efficiencies.
Care versus Cure
In both Canada and the United States, health system efficiency is the hottest new thing—hospitals are held to wide-ranging, measurable standards. This drive toward accountability and efficiency stems from a period of solid empirical research and practice, and has given us effective treatment, powerful drugs, and the ability to prevent illness in the first place. Patient care, though, takes effort that cannot always be planned for or measured. Hospitals have had to adjust to meet strict performance benchmarks in order to survive.
But it was not always so.
The Hotel Dieu, or “God’s Hostels”—early hospitals arising from monastic infirmaries that attended to the physical and spiritual needs of the poor and sick—grew over time in France and its colonies, run by fleets of highly skilled nun-caregivers. But with a growing understanding of the body through increasing experimentation, doctors began to wrest control of medicine from the strong-willed nuns. Most patients could offer little reward to this new dominant cohort of physicians. They did, however, function as helpful subjects on which to build a base of evidence in medical science, much to the horror of the church. A line of distinction was drawn by the secular medical establishment, separating care and cure.
Nuns and physicians waged a lengthy battle, carried on under the shadow of the French Revolution. Though scientific medicine was gaining rapid steam, the French government allowed the nuns to continue operating until France entirely secularized its hospital system in the early 1900s. With this transition, concepts perhaps too close to religion for comfort, such as anima and spiritus, were exiled from healthcare, along with the monks and nuns and their heretical pre-modern practices.
Community and Caring: The Way of Sweet’s Medicine
Sweet looks back into this long history in search of the thread connecting Laguna Honda and her deep desire to be a better healer. She finds that the root of today’s healthcare began in communities that shared the solitary goal of extending care, or hospitality, to those who needed it, regardless of their station in life. This vital element is what differentiates Laguna Honda from other modern institutions served by western medicine. To understand why a community setting is an ideal place to facilitate healing, Sweet again delves into language to reveal a term we often take for granted: community. The idea is best understood by its poetic beginnings: communio, “to build a wall around,” and munis, “those who share a gift in common.” At Laguna Honda, Sweet confides, “sharing made us a community.” She is describing both the patients and the staff, janitors and administrators, and all the groups occupying its open breezeways, playing poker games, and furtively smoking together in stairwells.
An analogy for this community comes by way of Sweet’s pilgrimage along the Camino de Santiago, where she grasps the power of hospitality and charity, demonstrated in the willingness of hosts to feed and house tired, blistered travellers. Reflecting on her role as pilgrim, she realises that the community of her hospital is a similar to those that she witnesses forming along the Camino. Every pilgrim plays a role, sometimes interchanging, all dependent on one another.
To understand this dynamic we need to explore the third key principle driving Laguna Honda, that of charity. The term originates in the tender caritas, “dearness”: the actions expressing God’s love. Charity fits squarely into hospitality and community; it happens both inside of, and for the benefit of, communities—both the givers and the beneficiaries. Medieval practitioners believed that caring for the sick poor created a bond of love that draws us closer to God. In this way, charity also assuages eleos, the feeling of pain caused by the sight of some evil that befalls one who doesn’t deserve it. Following the etymological breadcrumbs, we learn that eleos becomes the French aumone, and in English? Alms.
Laguna Honda’s alms reflect this assuaging of pain; the need to be charitable coming from society’s inability to witness injustice. The miracle is that, in a largely secular society, the community (in this case, San Francisco, but also other large swaths of society) still support charity and believe it is a priority to care for the vulnerable. We give money to international aid, serve in street outreach, establish AIDS/HIV clinics, and give to food banks. Charity is often inefficient, and we know it. Many forms do not deal with the root causes of injustice, but they do provide a balm of hope and relief in moments of need. It is “a complicated pleasure,” the relief that we experience, but these actions at their core demonstrate that we hold the other dear.
A Green Machine: Treating the Whole Person
Today the body is viewed as a machine that hums along and can, under the right conditions, be fixed. Pre-modern practitioners viewed every person as having veriditas, a “greenness,” that when properly nurtured allowed the body to heal itself, and needed to be attended to alongside the treatment of the immediate condition. This required attention to the physical and spiritual environment of the patient to allow the body’s natural, God-given defenses to kick in. “I stepped back and focused on the environment surrounding my patient”: Sweet begins to look for anything interfering with her patients’ healing process; pruning back the vines, letting the light in, and unleashing each patient’s veriditas.
The story of a woman named Terry illustrates this “greening” perfectly. Admitted from the streets of San Francisco’s rough Tenderloin neighbourhood, Terry’s infections are so advanced she is sent to Laguna Honda from the general hospital as a palliative case. Dr. Sweet considers her living situation, her pallid skin tone, and long history of drug abuse. Dr. Sweet ponders Hildegard’s pre-modern approach and begins to facilitate the activation of Terry’s unique veriditas, a process that takes two years of careful nurturing. As long as Terry feels a stronger pull toward the streets than to becoming healthy, Dr. Sweet knows no long-term change will occur. Bedbound, on her stomach constantly due to the aggressive and deep infection around her spine, Terry longs to go outside. When this request is met, she slowly shifts from despondency to a healthy annoyance with her situation. The community at Laguna Honda eventually draws Terry in, and the body that has been holding her captive begins to respond and come to life.
Open Wards, Community and the Myth of Modern Privacy
If community is so valuable, and open wards are so effective, where did they go? Each of us would likely profess a preference for our own room, a quiet and, most importantly, private space. Part of the answer lies in the birthing of the institution and the clinic over the eighteenth century, when hospitals began to merge with scientific medicine. Hospitals remained an important part of the social landscape, situated within the larger community, often closely connected to the church, but separated enough to prevent the spread of illness. During an outbreak, public health and social medicine sought to both separate and protect. Over time, when the great epidemics calmed, the principles and architecture of this spatial exclusion from the community remained.
Jeremy Bentham’s eerie Panopticon, originally designed with prisons in mind, began to gain a foothold with those responsible for overseeing large populations. The structure of “omnipresence” Bentham envisioned provided the healthcare community with knowledge of “contacts, contagions and proximity—assuring surveillance both global and individual.”
The result of the drive to “divide space and keep it open” for the purposes of quarantine and supervision was an internment from participating in community and the health-giving life therein.
Quiet: Hospital Zone
In 1890, S.D. Warren wrote The Right to Privacy, arguing that each person has the right to “keep a domain around us of our choosing.” Think again about your last overnight hospital stay—private rooms have become the desirable norm for many understandable reasons, one of them being the protection of dignity and privacy. Dr. Sweet observes, however, that with technology everywhere, patients in private rooms don’t get much of either. Perhaps, amidst this new hyper vigilance toward privacy and autonomy, the intangible thing that Hildegard nurtured, and which Dr. Sweet looked for on the autopsy table, has been lost.
Perhaps a reorientation of our view of privacy is needed. In Privacy and Freedom, Alan Westin suggests that there are not one, but four stages of privacy: solitude, intimacy, anonymity, and reserve. Intimacy is part of what makes Laguna Honda special. Within its large community of breezeways and open wards, individuals can be known and “held dear” by both caregivers and fellow patients. The physical spaces of the hospital provide for openness and transparency; its attentive staff, hidden garden benches, and group activities allow for groups to form or for solitude when it is needed. Staff can effectively manage “contacts and contagions,” while patients are able “to keep a domain around [them] of their choosing.”
Health systems need to be fairly utilitarian and mechanistic to properly cure based on well-established evidence. They should also, however, give a wide berth to the occasionally impractical, those efforts that seem inefficient or extravagant. These are the things, Sweet says, that allow veriditas to be re-infused into the bodies and spirits of her patients. These “efficient inefficiencies” insert green life back into systems—whether a whole healthcare system, the elements that work from the cell, to the organ, to the mind, restoring wholeness and function.
How do we hold on to those valuable inefficiencies—the little practices that help some patients get out of bed in the morning? Who bears that burden in a system that venerates outcome benchmarks and quarterly performance metrics? In many cases, patient care is maintained despite these centuries of upheaval by the same caregivers who fought against the French medical establishment in the late 1700s—once predominantly nuns, now they are our nurses. As hospital administrations push for efficiency, and time and resources are pressed, nurses pick up the slack again and again.
One veteran nurse says that what she does is simply “intuitive”—it can’t be measured or quantified: “Society doesn’t have a metric for human dignity.” Reflecting on balancing the technical and caregiving aspects of her work, she emphasizes that “you can learn everything there is to know about blood pressure and cardiac output, but if you aren’t observant enough to brush the white hair off your elderly patient’s favourite dark purple fleece, the other stuff doesn’t matter—they lose their personhood.” Upholding human dignity is what Laguna Honda does immeasurably well. We are all, in fact, largely still cared for by nurses and doctors who were motivated by compassion and eleos to enter their demanding professions. Even when cure is not possible, these keen observers and attendants can pull out a patient’s humanness and dignity from illness and vulnerability. This is caritas—dearness—and whether this is the intent or not, patients are reminded of their inherent value, that they have been made in the image and likeness of God.
Our Way Forward
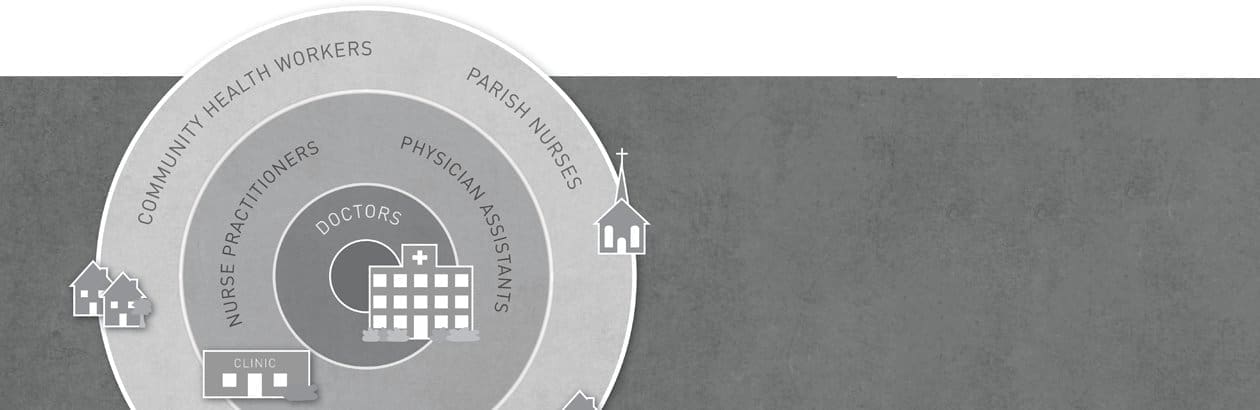
Many doctors profess that they are shocked at how hands-off their medical training and practice is compared to what they were expecting and hoping for as young students. This trend is shifting today thanks to newer medical training that seeks people who can connect with both patients and colleagues, work in teams, and understand the environmental contexts of the patients they see. In Canada and the United States, medical and nursing schools are changing both the methods and the places in which students train. Courses like “Doctoring” at UC Davis teach physicians to sit and really listen to the patient, to look up from the clipboard or computer screen, see the person in front of them and discern what they see. The medical community is striving to recruit and train physicians who can think both analytically and empathetically. Schools look not only for high test scores but the ability to think in an integrated manner: Where is this patient from? What is their affect like right now? How can we prevent this problem from happening again?
Nurses, thankfully, are being brought further into decision-making while physicians are consulting more across teams. Together, they ensure that their patient is treated as a whole person, not a checklist. Community-based care has become a priority as our population ages in places where complex health services simply aren’t available. Implementation of these new modes of care has been fraught with challenges, but we have turned a corner, culturally, with the realization that patients need to be observed within a community, not a vacuum.
These changes reflect society’s realization that we really did lose something despite great gains in quantitative efficiency and modernized medicine. Sweet sought that “something” in her chronicles, and she is one of the few western practitioners able to practice in a place where the old and the new exist together. Her spiritually rooted replication of pre-modern medicine is a challenging concept to execute within today’s secular environment. The very effectiveness of Hildegard’s medieval practice was rooted in the faith that God is an active and present part of the healing process, that charity is the core motive, and that dearness binds the doctor and the patient. Even in a secular, system-driven society, though, we can find those “otherworldly” motives everywhere in the delivery of care and the ongoing search for cure. Nurses continue to extend themselves on behalf of patients despite piles of charting waiting for them; physicians sit and listen despite the pressures of the fifteen-minute billing time slot. It is these “counterrevolutionary individuals,” the ones determined to act between the lines of dictated treatment plans, who continue Hildegard’s legacy, bringing anime and spiritus back to the hospital and the bedside.