Table of Contents
Table of Contents
Key Points
- This paper discusses findings from a fall 2024 poll, conducted by the Angus Reid Institute in partnership with Cardus, and other available data and research, about Canadians’ level of support for MAiD. It also provides data on how MAiD affects people with disabilities and affects Canadians’ trust in healthcare.
- The majority of Canadians say they are in favour of MAiD, but this support may be hollow given other data showing that Canadians do not actually know what constitutes MAiD, or who qualifies for it.
- What most Canadians support, in fact, is MAiD for exceptional or last-resort cases, criteria that are much narrower than current law.
- Fifty-seven percent of Canadians living with severe disabilities say they experience barriers or discrimination in healthcare. Forty-five percent of healthcare workers say that people with disabilities receive “poor” or “terrible” healthcare in Canada.
- Three in five Canadians agree with the statement “I’m worried about financially or socially vulnerable people considering MAiD because they can’t access adequate, quality care.”
- Health Canada reported that 163 people with a disability did not receive disability support services and received MAiD in 2024, and an additional 239 persons required such services, but it is unknown if they were received. The Office of the Chief Coroner of Ontario has documented cases in which MAiD requests appear to have been driven by untreated mental illness, lack of adequate housing, or caregiver burnout, and yet these Ontarians went on to die by MAiD.
- Forty percent of Canadians are in favour of prohibiting doctors from raising the subject of MAiD with their patients unsolicited; by contrast, 43 percent say that doctors should be free to do so. (Canada’s MAiD law does not prohibit doctors from raising the subject unsolicited, unlike some international jurisdictions.)
- Fifty percent of Canadians living with severe disabilities, and 38 percent of those without disabilities, agree that patients may feel pressured to choose MAiD if this subject is raised by their doctor.
- Canadians living with severe disabilities are twice as likely as Canadians without severe disabilities to “strongly agree” that some healthcare facilities should be MAiD-free spaces.
Introduction
In the debates about euthanasia and assisted suicide, or medical assistance in dying (MAiD), one of the key concerns is the impact that MAiD may be having on Canadians living with vulnerabilities. 1 1 Canada has adopted the language of “medical assistance in dying” or “MAiD” to refer to both euthanasia and assisted suicide. Very few cases in Canada are “self-administered” MAiD (assisted suicide), however. Quebec does not allow self-administered MAiD at all, and Saskatchewan indicates that MAiD by oral consumption is not available. See also the Saskatchewan Health Authority webpage: https://www.saskhealthauthority.ca/your-health/conditions-illnesses-services-wellness/all-z/medical-assistance-dying/accessing-maid-saskatchewan. As such, MAiD in Canada is “clinician-administered” MAiD (euthanasia) in all but a very few cases. This paper primarily uses the term “MAiD,” in large part because this is the term used in the Angus Reid Institute polls discussed in this paper. For more on the legislative and regulatory frameworks of MAiD, see Raikin, “From Exceptional to Routine.” Complete citations are provided for all sources at the end of this report. Do those living in difficult socioeconomic circumstances or those experiencing barriers to quality care sometimes opt for a premature death from MAiD because of those difficult circumstances? Do those living with disabilities—who are already more likely to experience economic, social, and healthcare-related discrimination—opt for “assistance in dying” because of inadequate assistance in living?
The courts and legislature have acknowledged a concern for how MAiD might impact Canadians with vulnerabilities. In 1993, the Supreme Court decision Rodriguez v. British Colombia (Attorney General) upheld the prohibition against euthanasia and assisted suicide on the basis of the state’s objective to protect the vulnerable and, more generally, to “protect and maintain respect for human life.” 2 2 Rodriguez v British Columbia (Attorney General), p 523 at a. Further, the justices wrote in Rodriguez, the full prohibition against assisted dying was “not overbroad since there is no halfway measure that could be relied upon to achieve the legislation’s purpose fully.” 3 3 Rodriguez v British Columbia (Attorney General), p 523 at b. In other words, there was no way to keep vulnerable Canadians safe without keeping assisted dying fully illegal.
Yet in the 2015 Supreme Court decision Carter v. Canada (Attorney General), the court struck down the Criminal Code’s complete prohibition of euthanasia and assisted suicide. It agreed with the lower court trial judge “that a permissive regime with properly designed and administered safeguards was capable of protecting vulnerable people from abuse and error,” 4 4 The evidence that the trial judge used to reach this conclusion is contested, however, as Alexander Raikin reviews in more depth in “In Contrast to Carter.” and it ruled that a blanket ban of MAiD was broader than necessary to protect vulnerable persons. 5 5 Carter v Canada (Attorney General), 2015. For detail on the Carter decision, see Shariff, “Carter v Canada” or Grant, “Legislated Ableism.”
Parliament was thus tasked with responding to the court’s decision. It did so by carving out an exception in the Criminal Code to allow patients to receive and clinicians to provide euthanasia and assisted suicide, but balancing access to this exception with the protection of those living with vulnerabilities. This legislation, and the government’s own statements, explicitly recognize a need to protect vulnerable persons. 6 6 Bill C-14, An Act to Amend the Criminal Code and to Make Related Amendments to Other Acts (Medical Assistance in Dying); Bill C-7, An Act to Amend the Criminal Code (Medical Assistance in Dying). But is this protection, in fact, working?
Many persons living with disabilities, as well as scholars, clinicians, and advocacy organizations, argue that it is not, and that vulnerable persons are feeling the effects of MAiD’s introduction—sometimes with fatal consequences. Expansions of MAiD have continued, however, and more and more Canadians are opting for a premature death, with social suffering and inadequate care a factor in many requests and provisions.
In the fall of 2024, the Angus Reid Institute (ARI) in partnership with Cardus conducted public opinion polling to better understand how vulnerability may be interacting with MAiD and what impact this may be having on Canadians, including those living with disabilities. ARI published two reports on this polling data, on November 21 and December 12, 2024. 7 7 In this paper, the poll itself is referred to as the ARI fall 2024 poll, and specific results reference the relevant reports: Angus Reid Institute, “Disability & MAID”; Angus Reid Institute, “Division over Aspects of Assisted Dying.”
This discussion paper engages with important findings from this poll, discussing them in the context of other literature and research relevant to the topic. First, this paper considers Canadians’ overall support for the MAiD law in the context of other research showing that what Canadians support is, in fact, MAiD for exceptional or last-resort cases, criteria that are much narrower than the current laws.
Next, the paper reviews the ARI data on Canadians with disabilities’ experience of the healthcare system and on Canadians’ concerns with how inadequate care and support may influence MAiD decisions. Available data from Health Canada and the Ontario Coroner’s Office, on the relationship between inadequate care and MAiD choices, are also considered.
Last, we review the ARI data on how MAiD may be affecting trust in healthcare, and examine Canadians’ views on such questions as whether doctors should be prohibited from raising the subject of MAiD unsolicited by their patients, and whether some healthcare facilities should be able to remain MAiD-free.
Overall, this paper highlights knowledge gaps in Canadians’ views on MAiD, and some of the specific concerns and challenges that Canadians living with disabilities face in relation to MAiD. This paper does not recapitulate the polling results in a comprehensive way, and readers are invited to refer to the Angus Reid Institute’s reports and detailed data tables.
Canadians Generally Support MAiD . . . But Do They Know What It Is?
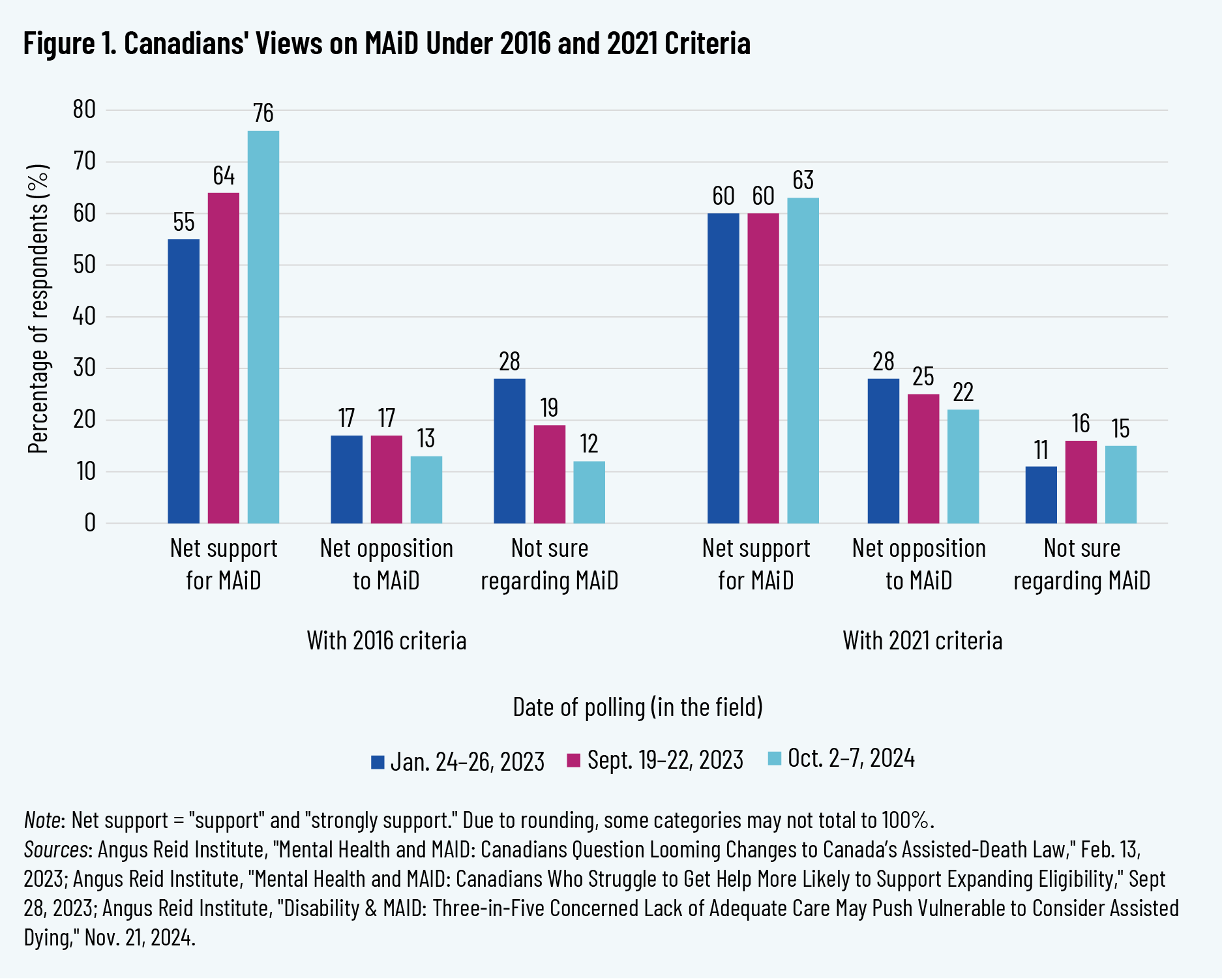
The ARI poll conducted in the fall of 2024 finds overall high levels of support for MAiD, under the original 2016 criteria (Bill C-14) and under the expanded 2021 criteria (Bill C-7). Support is somewhat lower for the 2021 expanded criteria (63 percent support) than for the 2016 criteria (76 percent support).
An increase in Canadian support can also be seen over time, when comparing the fall 2024 poll results to previous ARI poll results in September 2023 and February 2023. The percentage of respondents who answered that they were “unsure” if they supported or opposed the MAiD law has also declined somewhat, particularly for the 2016 criteria, from 28 percent in February 2023 to 12 percent in September 2024.
These data align with results from other public polling, such as that conducted by Ipsos on behalf of Dying with Dignity Canada, an organization with the goal of realizing and expanding assisted dying in Canada. 8 8 Ipsos and Dying with Dignity Canada, “Support for Medical Assistance in Dying in Canada.”
The ARI November report flags that those living with more severe disabilities are more likely to “strongly support” the 2021 MAiD criteria (37 percent), compared with those with no disability (27 percent) and the poll respondents as a whole (29 percent). 9 9 Angus Reid Institute, “Disability & MAID,” 12. For those living with either “moderate” or “less severe” disabilities, 30 percent strongly supported the 2021 criteria. ARI assessed the respondents’ degree of disability through questions on “the frequency and extent to which their disability/condition interferes with or limits their daily activities . . . to assign a level of ‘severity’ for analysis purposes” (p. 15).
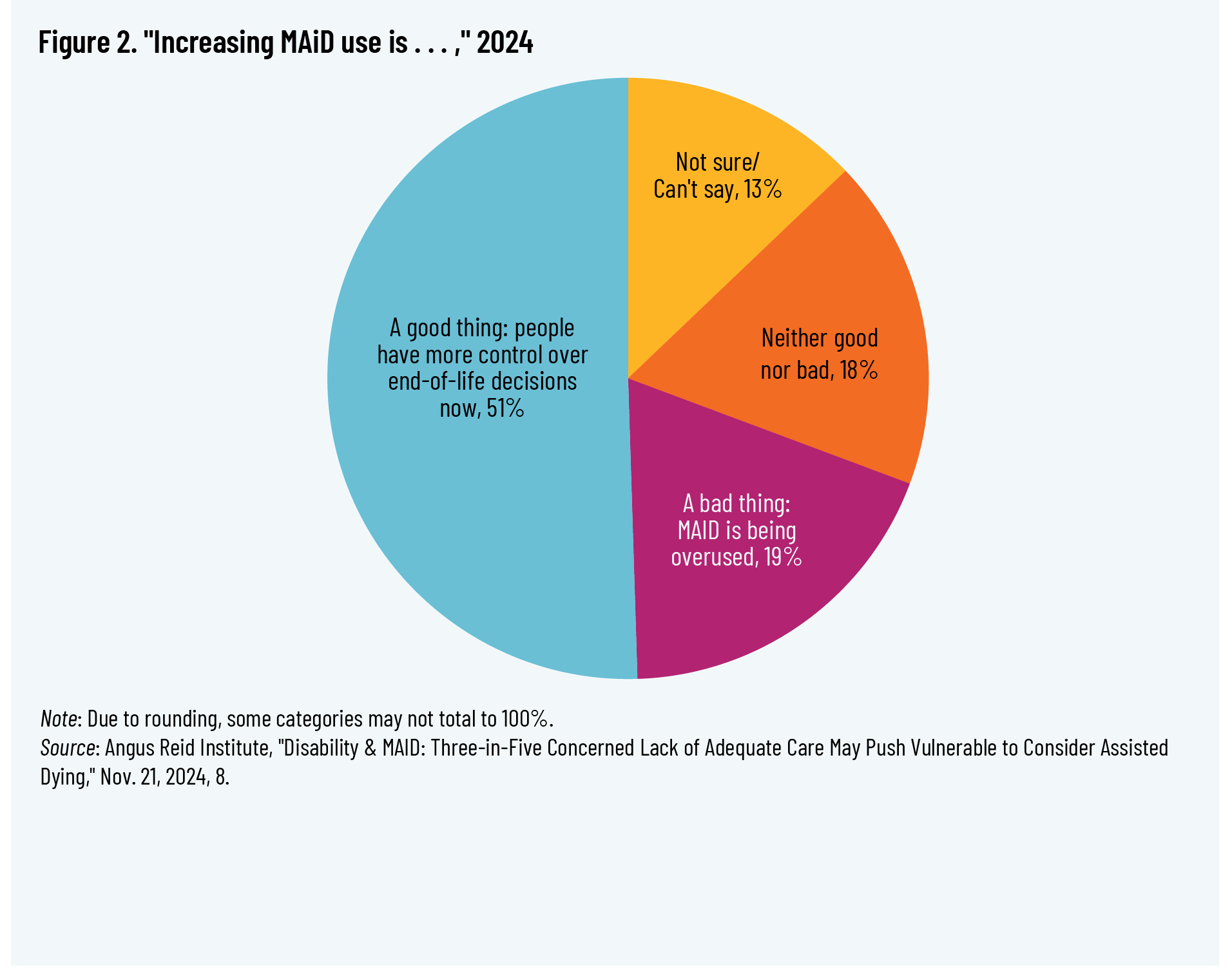
When asked about the increased use of MAiD in Canada, a slim majority of Canadians agreed that this was “a good thing: people have more control over end-of-life decisions now” (51 percent) as opposed to “a bad thing: MAiD is being overused” (19 percent). 10 10 The remaining respondents included 18 percent who said it was “neither good nor bad” and 13 percent who indicated “not sure/can’t say.” Angus Reid Institute, “Disability & MAID,” 7.
The breakdown of views for increased use of MAiD differs very little across provinces or between Canadians living with disabilities and Canadians generally. An exception is found in Quebec; here, the proportion of those who view increased use of MAiD as “a good thing” is significantly higher than in other provinces, at 67 percent, with only 11 percent viewing it as “a bad thing.” 11 11 Angus Reid Institute, “Disability & MAID,” 7.
Importantly, Canadians’ overall support for MAiD may be hollow given their lack of understanding of how MAiD operates and who qualifies for it. Tapp et al., for instance, found significant confusion among their own survey respondents as to what constituted MAiD and what did not, and what was legal in Canada and what was not. 12 12 Tapp et al., “Individual Characteristics.” Although the paper was published in 2025, the data come from a survey conducted between fall 2019 and winter 2020. More than a quarter of their respondents incorrectly conflated withholding treatment with MAiD, and nearly 40 percent incorrectly conflated continuous palliative sedation with MAiD. In light of the community-based sample’s limitations—which included being “largely comprised of women with a high level of education”—it was “possible that there was a systematic bias among the respondents, such that those who have more knowledge and interest in end-of-life practices may have been more likely to volunteer to participate.” The researchers thus indicated that the “confusion and lack of knowledge” about MAiD may be even more pronounced among Canadians writ large. 13 13 Tapp et al., “Individual Characteristics,” 7. The study was also limited due to being conducted only in Quebec.
Choi et al. surveyed 2,140 Canadians in 2024 on their knowledge of and stance toward MAiD. When asked if they “support or oppose allowing a person to receive MAID in Canada if all the conditions are met,” the majority of the respondents were supportive (73.3 percent), in line with other Canadian polling data, including ARI data. However, only a small minority of the respondents (12.1 percent) could correctly answer at least four of the five knowledge questions about the law, revealing major misunderstandings as to who is actually eligible for MAiD. 14 14 Choi et al., “When Medical Assistance in Dying Is Not a Last Resort Option,” 3–4.
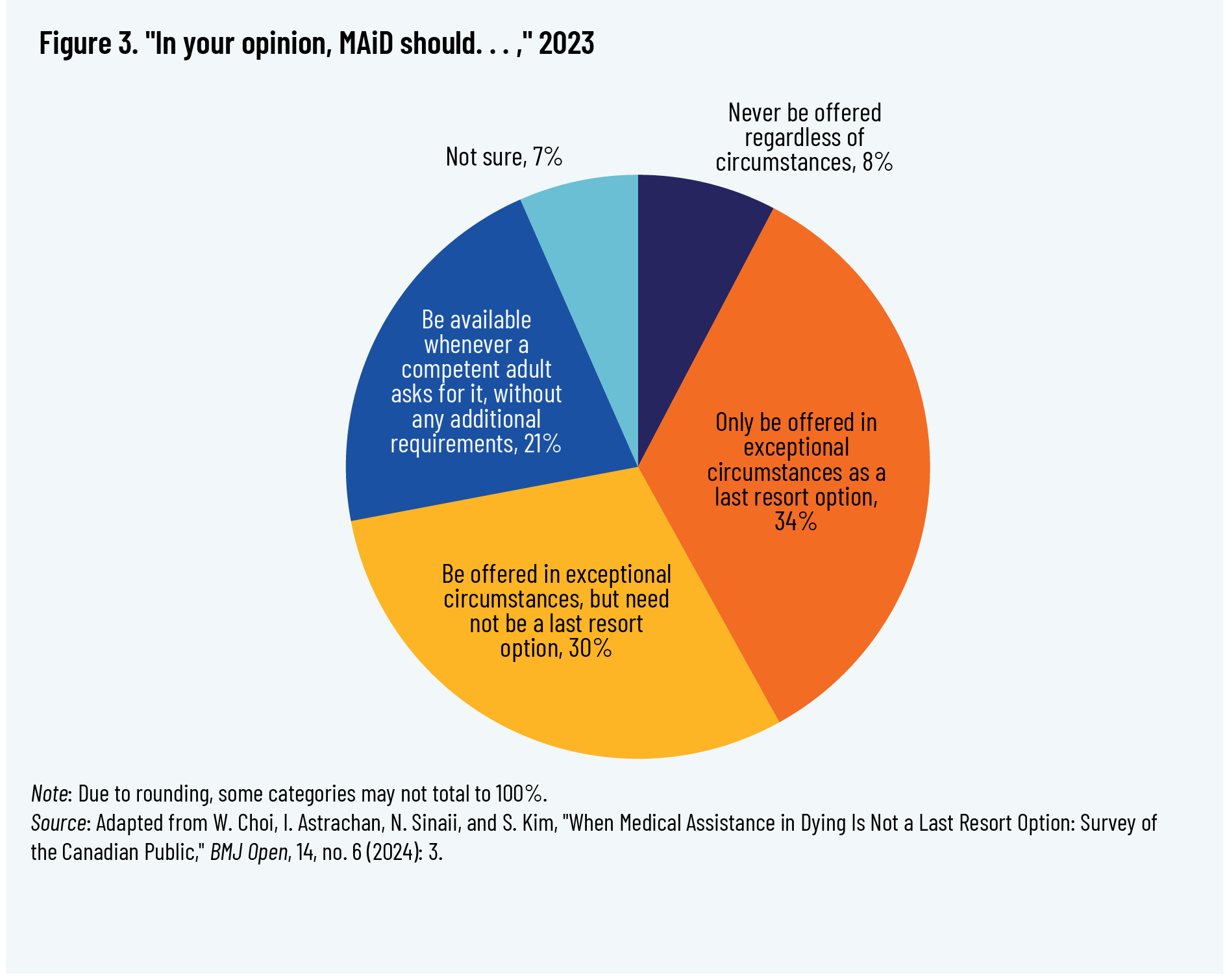
On specific eligibility questions, “only 19.2% of participants correctly answered that patients do not need to have a terminal illness to qualify for MAID, [and] 20.7% correctly answered that patients may refuse medically effective treatment and still qualify for MAID.” Further, over 60 percent of respondents agreed that MAiD was appropriate only for “exceptional situations,” with 34.3 percent agreeing that it should be only “a last resort option” and another 30.1 percent agreeing that it should be limited to “exceptional circumstances, but need not be a last resort option.” 15 15 Choi et al., “When Medical Assistance in Dying Is Not a Last Resort Option,” 3–4.
Respondents were also provided with four hypothetical scenarios of patients requesting MAiD. Although the patients could all qualify for MAiD under Canadian law, only a minority of survey participants (23–32 percent, depending on the scenario) correctly identified that the patients were eligible, and only a minority (23–32 percent, depending on the scenario) supported providing MAiD in these cases. The rationales given by the respondents for their lack of support in these scenarios were that the patient had the possibility of improvement with treatment or with further assistance, and that MAiD was not a last resort. A majority, across the scenarios presented, agreed with health provider decisions to decline to provide MAiD since it was not the last resort in that situation. 16 16 Choi et al., “When Medical Assistance in Dying Is Not a Last Resort Option,” 4.
In light of these findings, Choi et al. concluded that “although Canadians broadly express support for their MAID law, most do not support the practices that are (or scheduled to be) permitted by that law.” This raises questions for policymaking, with the authors asking:
First, why is there such a large gap between Canadians’ support for the MAID law in general and their support for specific implications and provisions of that same law? Second, how significant is it that the public do not seem to see this gap because they do not believe that the law is as permissive as it really is? Future research might focus on how an apparently popular idea—legalised MAID—came to be implemented in a way not supported by most Canadians. 17 17 Choi et al., “When Medical Assistance in Dying Is Not a Last Resort Option,” 6–7.
ARI polling in February 2023, conducted in partnership with Cardus, also found that Canadians generally accept the MAiD law but that the majority do not agree with specific practices that the law allows. For instance, the poll found that 65 percent of respondents agreed that “potential patients should have to exhaust ALL treatment alternatives before MAID is available,” compared to 24 percent who disagreed and 11 percent who were unsure. 18 18 Angus Reid Institute, “Mental Health and MAID: Canadians Question Looming Changes,” 9.
Canadians’ majority support for MAiD only as a last resort is incongruent with the law, which has never required that the patient have a terminal illness nor exhaust all treatment options. The “reasonably foreseeable death” requirement of 2016 was interpreted liberally by MAiD assessors and providers, with some providers approving MAiD for patients with a life expectancy of five to ten years. 19 19 See, for instance, Canadian Association of MAiD Assessors and Providers, “Clinical Practice Guideline.” This is in contrast to some international jurisdictions where legal assisted dying is limited to those with terminal diagnoses specifically, often with a specific prognosis (usually six months or a year). Canada subsequently removed the “reasonably foreseeable death” requirement in 2021, creating Track 2 MAiD.
Healthcare Deficiencies and MAiD: A Fatal Connection
How Canadians with Disabilities Experience Healthcare
The views and experiences of persons living with disabilities were a key focus of the fall 2024 ARI poll. It found that many Canadians report living with some sort of disability, ranging from 28 percent with a long-term mental health condition to 22 percent with chronic pain to “other serious concerns such as mobility issues (8 percent), hearing disability (8 percent) and vision disability (6 percent).” 20 20 Angus Reid Institute, “Disability & MAID,” 3.
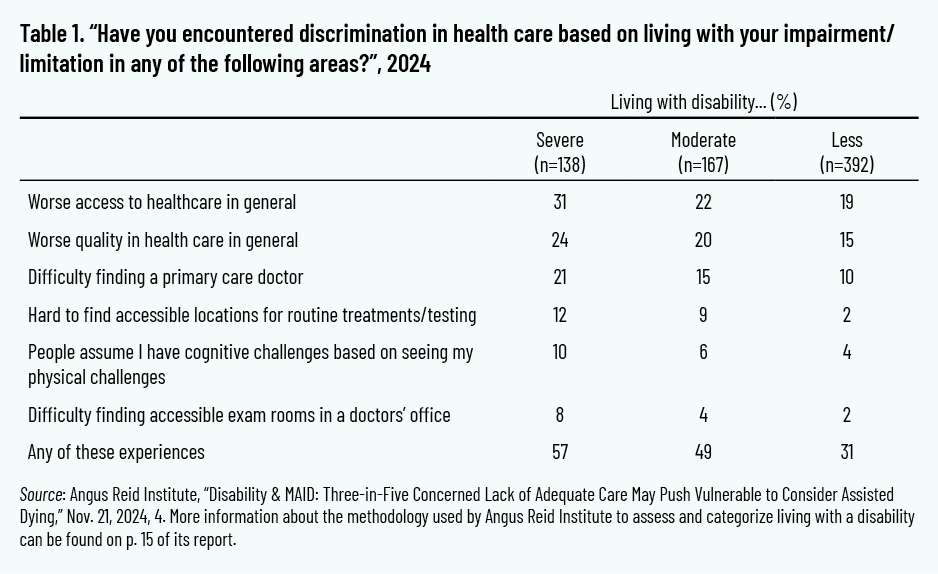
When asked about their experiences of healthcare, a majority (57 percent) of the subset of those living with disabilities that severely affect their day-to-day lives reported experiences of discrimination. Of this subset 31 percent believed that they had worse access to healthcare in general and worse quality in healthcare in general (24 percent) compared to persons without disabilities, and 21 percent reported that they had difficulty finding a primary care doctor. 21 21 Angus Reid Institute, “Disability & MAiD,” 4.
These findings should be considered in light of the limits of the sample, however. As ARI stated in its November report, its definition of disability is more expansive than that of Statistics Canada, for instance, which may account for the higher number of respondents self-identifying with a disability in the ARI poll, compared to surveys conducted by Statistics Canada. 22 22 Angus Reid Institute, “Disability & MAiD,” 15.
A caveat is also always needed for self-reported data on the subject of disability, as considerable variation may occur in how respondents define and thus respond to disability-related questions. The data are also limited in what they can tell us about how Canadians living with different types of disabilities, and multiple disabilities, experience the healthcare system and possible discrimination. For instance, as described above, mental illness and chronic pain were the disabilities most reported by the poll respondents, whereas “mobility issues” were reported by a much smaller number. Thus the findings may not apply to those whose disabilities were underrepresented in the sample. Larger samples of those living with different types of disabilities would be necessary to gain a clearer picture of healthcare experiences and views on MAiD. 23 23 Researchers at Statistics Canada have examined accessibility concerns and experiences of people with various types of disability, but the study is not about healthcare specifically. Hachouch et al., “Barriers to Accessibility Related to Behaviours, Misconceptions or Assumptions.”
Canadians’ Worries About Inadequate Care and MAiD
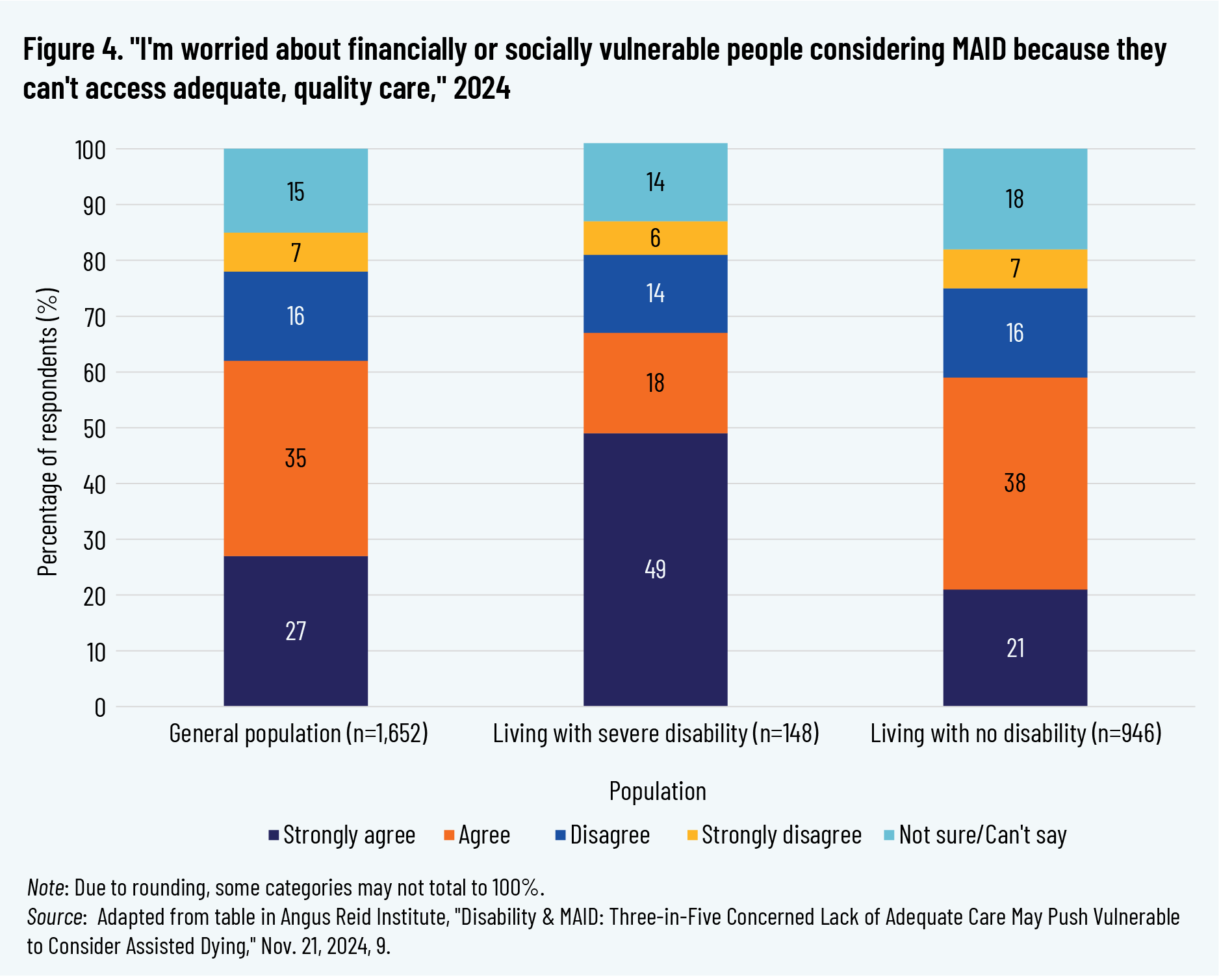
Canadians’ views on the MAiD law should be understood in the context of their concerns about how inadequacies in care may influence a patient’s decision to receive a MAiD death. In ARI’s fall 2024 poll, three in five respondents (62 percent) agreed with the statement “I’m worried about financially or socially vulnerable people considering MAID because they can’t access adequate, quality care.” Of the subset of respondents living with severe disabilities, 49 percent “strongly agreed,” compared to 27 percent of all respondents. 24 24 Angus Reid Institute, “Disability & MAID,” 9. Given that this subset was also more likely to report negative and discriminatory experiences of healthcare, their concerns about how inadequate care may impact MAiD choices are both unsurprising and troubling.
Similar concerns were expressed in the 2023 ARI poll. Here, only 25 percent of respondents said they supported MAiD for cases in which a person “can’t get access to medical care.” Only 9 percent supported MAiD for those who “cannot find affordable housing,” and 24 percent or less, depending on the particular scenario the poll presented, supported MAiD for a mental health related reason. 25 25 Angus Reid Institute, “Mental Health and MAID: Canadians Question Looming Changes,” 7.
Healthcare Workers’ Concerns
The ARI poll included a sample of 468 healthcare workers. Forty-five percent of these respondents indicated that they thought those living with disabilities in their province received “poor” or “terrible” care, as opposed to “good” (34 percent) or “excellent” care (3 percent). When asked to compare how persons living with disabilities were treated in healthcare, compared to Canadians generally, these respondents raised concerns about worse or much worse speed of access to care (38 percent), quality of care (36 percent), and seriousness with which the concerns of patients living with disabilities were taken (42 percent). Forty percent of these healthcare workers felt unequipped to support the healthcare needs of those living with disabilities. 26 26 Angus Reid Institute, “Disability & MAID,” 5–6. There are limitations to this sample of healthcare workers: It included very few doctors (3 percent of the sample, approximately 14 cases), nurses were 21 percent of the sample, and the largest segment of the sample was “other,” at 60 percent. This significantly limits how well the poll’s results apply to doctors, nurses, and other types of healthcare workers that were underrepresented in the sample. Fifty-three percent of the sample formerly worked in healthcare, which may affect the results as to current challenges or relatively new challenges such as MAiD. See also the associated table of results with healthcare workers at Angus Reid Institute, “MAID Spectrum HCW Tables.”
Media Reports on Inadequate Care and MAiD
Due to media reporting, we know of some cases in which inadequate care or inadequate disability supports have contributed to MAiD decisions. There may also have been cases that have gone unreported.
- Sean Tagert, an ALS patient denied additional home care, chose MAiD in 2019 after being forced into an institution at an extended distance from his son. 27 27 CBC News, “B.C. Man with ALS Chooses Medically Assisted Death.”
- Donna Duncan’s receipt of MAiD in 2021 was heavily criticized by her daughters, who emphasized Donna’s chronic lack of psychiatric care. 28 28 Favaro, “Police Investigating Medically-Assisted Death.”
- An Ontario woman known by the pseudonym Sophia received MAiD in 2022 after years of struggling to receive care for her multiple chemical sensitivities; specifically, to secure housing to accommodate her disability. 29 29 Favaro, “Woman with Chemical Sensitivities.”
- Melissa Ellsworth applied for MAiD in 2023 after years of fighting for treatment for workplace injuries, arguing that there were options to relieve her pain and support her quality of life but that she could not afford to access them without provision through workers’ compensation. 30 30 Ayers, “Cape Breton Woman Seeks MAID.”
- Normand Meunier was a paraplegic whose four-day wait on a stretcher in an emergency room resulted in severe pressure wounds, despite his partner repeatedly requesting that hospital staff provide a pressure-relieving mattress to prevent sores. Meunier subsequently opted for MAiD in 2024 as a result of the pressure sore; his care is under investigation by a Quebec coroner’s inquiry as of spring 2025. 31 31 Watts, “Quebec Coroner Orders Public Inquiry”; Watts, “Quadriplegic Quebec Man Chooses Assisted Dying.”
- Jennifer Brady applied for MAiD in 2024 after spending years fighting for the care and procedures to manage her chronic condition. 32 32 MacIvor, “A Halifax Woman Has Spent Years Fighting.”
Further discussion of disturbing cases related to disability are also discussed in academic publications. 33 33 See, for example, Coelho, “Disability and MAiD”; Stainton, “Disability, Vulnerability and Assisted Death”; Grant, “Legislated Ableism.”
Unfortunately, due to limited data collection, we do not know how prevalent this issue is. But what data are available present cause for concern, as discussed below.
Government Reports on Inadequate Care and MAiD
Health Canada
Health Canada’s annual reports on MAiD include limited data on MAiD recipients who self-identified as having a disability, and whether they had access to disability support services. The Fifth Annual Report, for instance, recommends “caution” with regard to its 2023 data on disability, due to inconsistencies in the data collection processes and definitions. It also states, “Information about access to palliative care and disability supports is important to ensure that MAID is not being sought because of a lack of options for end-of-life-care or support services.” Yet the report goes on to say that “most MAID recipients who required either palliative care or disability support services received these services” and fails to express concern about those who did not receive such services. Of those who received MAiD and self-reported a disability, the report states that 432 persons in 2023 required but did not receive disability support services. 34 34 Health Canada, Fifth Annual Report, 8, 13, 47, 49. The Sixth Annual Report says there were 163 persons requiring but not receiving disability supports, as well as 239 cases where services were required, but it is unknown if they were received. 35 35 Health Canada, Sixth Annual Report, 52.
In many cases, we simply do not know whether disability support services were required. The data for 2024 do not indicate whether disability supports were necessary for 13.6 percent of those who received Track 1 MAiD and who identified as having a disability, or for 8.7 percent of those who received Track 2 MAiD and who identified as having a disability. 36 36 Health Canada, Sixth Annual Report, 37. Although the number of Track 2 cases are smaller, because they do not have a “reasonably foreseeable death” and thus qualify on the basis of having a disability, the fact that MAiD providers did not determine whether disability supports were needed is disconcerting.
Further, the annual reports fail to explain the limitations of these data—specifically, that they cannot tell us anything about the adequacy of these supports. For those who did receive disability support services, we have no quality measures, and minimal data are collected as to duration of the support. More importantly, we do not know if the received disability supports were considered adequate by the recipients, or if they were received in a timely manner or for as long a duration as needed.
All together, Health Canada’s data, with their limitations and notable silences, should raise, not assuage, concerns about how adequacy of care is affecting MAiD decisions.
Ontario’s MAiD Death Review Committee
Unlike other jurisdictions with legalized assisted death, Canada did not create a national review body to monitor MAiD and enforce compliance. Although Health Canada provides some reporting, its mandate does not extend to monitoring or compliance. 37 37 Kotalik, “Monitoring of MAID.” Some provinces have internal review mechanisms, and some have a degree of public reporting or transparency. Quebec, exceptionally, has a commission that reviews cases and provides public reporting on MAiD, including on compliance with the law, although the reports are unclear about how compliance issues are resolved or what consequences they result in, if any. 38 38 Government of Québec, Commission sur les soins de fine de vie, La Commission sur les soins de fin de vie.
Some of the more robust reviews of MAiD practice in Canada have been conducted through the Office of the Chief Coroner of Ontario, which established a MAiD Death Review Committee in early 2024. 39 39 MAiD Death Review Committee reports are not available through the Coroner’s Office website but have been widely circulated through other sources. The Coroner’s Office found that Track 2 MAiD recipients are much more likely to come from highly marginalized areas as compared to Track 1 recipients or the general population. (Marginalization was assessed using an index developed by Public Health Ontario, the Centre for Urban Health Solutions, and St. Michael’s Hospital that uses metrics relating to each community’s material resources, households and dwellings, age and labour force; and racialized and newcomer populations.) 40 40 Government of Ontario, Office of the Chief Coroner, Medical Assistance in Dying (MAiD).
Further, the MAiD Death Review Committee has documented disturbing cases, including those in which patients received MAiD despite inadequately assessed or treated mental illnesses that appeared to be driving the MAiD request, and those in which patients requested and received MAiD due to housing vulnerability. 41 41 MAiD Death Review Committee, Office of the Chief Coroner, MAiD Death Review Committee (MDRC) Report 2024 - 2; MAiD Death Review Committee, Office of the Chief Coroner, MAiD Death Review Committee Report 2024 - 3. These issues become heightened in cases where patients received MAiD in a highly expedited manner, such as on the same day as the MAiD assessment, or on the next day.
One case discussed in the fourth committee report was of “Mrs. B,” whose spouse and caregiver appeared to be experiencing caregiver burnout and who initiated the MAiD request on her behalf. In her first MAiD assessment, Mrs. B expressed her desire to receive palliative and hospice care instead of MAiD. The next day, however, Mrs. B and her spouse presented at the emergency department; she was denied hospice care and discharged back home. Then, “on the same day, Mrs. B’s spouse contacted the provincial MAiD coordination service requesting an urgent assessment. A different MAiD assessor from the previous day completed a primary assessment and determined Mrs. B to be eligible for MAiD.” When the initial MAiD assessor was contacted and expressed concern as well as a desire to reassess Mrs. B, this assessor was denied access. A third assessor was then arranged for, approving Mrs. B for MAiD by means of a virtual assessment. “The provision of MAiD was completed later that evening.” 42 42 MAiD Death Review Committee, Office of the Chief Coroner, MDRC Report 2024 - 4, 3, 21–22. The review committee highlighted the role that the barrier to in-patient palliative care or hospice care played in this MAiD death, noting that
poor quality end-of-life care potentially impacted the request for a brief MAiD provision timeline (i.e., concerns of burnout went unaddressed, advocacy for the necessity of admission to in-patient palliative care or hospice was not evident). Some members [of the committee] expressed their concern that access to MAiD was more easily organized and accessible in this circumstance than the previously requested and preferred option for end-of-life care. 43 43 MAiD Death Review Committee, MDRC Report 2024 - 4, 22.
Ableism in Healthcare
Considering the impact of ableism on healthcare is critical to understanding disability experiences in healthcare. Ableism refers to discrimination against those living with disabilities based upon seeing disability as a flaw and thus seeing disabled persons as flawed. Disability scholar Heidi Janz describes how “ableism becomes systemic as patterns of discriminatory and exclusionary practices against people with disabilities are entrenched in sectors that are fundamental to societal membership, such as education, employment, and housing.” 44 44 Janz, “Plagued to Death by Ableism,” 137.
Persons with disabilities face considerable barriers to accessing healthcare and can experience adverse health outcomes as a result. 45 45 De Vries McClintock et al., “Health Care Experiences and Perceptions”; Lagu et al., “‘I Am Not the Doctor for You.’” A 2025 analysis using 2017–18 Statistics Canada survey data identified Canadians with disabilities as four times as likely to have unmet healthcare needs, compared to Canadians without disabilities, confirming similar findings on healthcare disparities for persons with disabilities from other Canadian and international research. 46 46 Pucchio, Stranges, and Ali, “Disability and Unmet Need for Health Care in Canada.” For instance, persons with disabilities were in “triple jeopardy” during the COVID-19 pandemic due to “the increased risk of poor outcomes from the disease itself, reduced access to routine health care and rehabilitation, and the adverse social impacts of efforts to mitigate the pandemic.” 47 47 Shakespeare, Ndagire, and Seketi, “Triple Jeopardy,”1331. Janz describes, for instance, how provincial Critical Care Triage Protocols “prohibited many disabled people from receiving critical care in the event that a surge in severe COVID-19 cases outstripped available resources.” Janz, “Plagued to Death by Ableism,” 137.
A key concern that disability advocates raise about MAiD is how it interacts with ableism within society in general and healthcare specifically. 48 48 As this paper treats this topic very briefly, readers would benefit from fuller treatments within the scholarship, including Janz, “Plagued to Death by Ableism”; Stainton, “Assisted Life Before Assisted Death”; Grant, “Legislated Ableism”; Frazee, “MAID Resistance in Canada”; Janz, “MAID to Die by Medical and Systemic Ableism.” Disability organizations such as the Council of Canadians with Disabilities, Inclusion Canada, and ARCH Disability Law, among many others, have brought these concerns to light in their advocacy, public statements, and court actions. 49 49 ARCH Disability Law Centre, “Submission to Special Joint Committee on Medical Assistance in Dying”; Inclusion Canada, “Bill C-7 Through a Disability Lens”; Inclusion Canada, “Press Release: Disability Rights Coalition.”
As disability scholar Tim Stainton argues, “MAID as currently constituted increases the vulnerability of disabled Canadian[s] and . . . will lead to unwanted and unnecessary shortening of lives due to poverty, ableism and a lack of appropriate and sufficient disability supports.” 50 50 Stainton, “Assisted Life Before Assisted Death,” 311. Asada et al. point to concerns with potential areas of “mismatch” between healthcare needs and available access among those who may request MAiD, including challenges with wait times, uneven drug insurance coverage, accessibility of palliative care, and disability supports. 51 51 Asada et al., “Importance of Investigating Vulnerabilities.”
Research on biases among healthcare practitioners, in terms of how they view the quality of life of persons with disabilities, shows how the presence of negative attitudes can result in barriers to care. 52 52 Lagu et al., “‘I Am Not the Doctor for You,’” 6–7. As discussed in a 2021 study, 82.4 percent of surveyed American doctors believe that persons with disabilities have a worse quality of life than persons without one. 53 53 Iezzoni et al., “Physicians’ Perceptions of People with Disability.”
Scholars identify this as the “ableist conflation,” whereby clinicians equate disability with pain and suffering and make quality-of-life assumptions on that basis. 54 54 Binkley, Reynolds, and Shuman, “From the Eyeball Test to the Algorithm”; Reynolds, “‘I’d Rather Be Dead than Disabled.’” Such bias seriously affects communication between practitioners and patients and can adversely affect patient health outcomes. 55 55 Reynolds, “‘I’d Rather Be Dead than Disabled.’” It may influence how doctors present MAiD as an option to persons living with disabilities. The fatal consequences of these care gaps and ableist biases can be seen playing out in the cases discussed earlier in this paper.
Legislated Ableism
Significantly, the 2021 expansion of MAiD to persons who are not dying occurred against the backdrop of the COVID-19 pandemic, which itself had profound and often lethal consequences for Canadians living with disabilities, as described above. 56 56 Whitelaw, Lemmens, and Van Spall, “The Expansion of Medical Assistance in Dying”; Grant, “Legislated Ableism,” 263–65; Janz, “Plagued to Death by Ableism”; Shakespeare, Ndagire, and Seketi, “Triple Jeopardy.” In this context, the federal government significantly expanded MAiD eligibility in Bill C-7 (Track 2), despite opposition from major disability rights organizations, scholars, and activists. Disability advocates and organizations described feeling “sidelined, stonewalled, patronized and betrayed at every turn” as the bill worked its way through Parliament despite their opposition. 57 57 “About–Disability Filibuster,” Disability Filibuster. Practically speaking, the pandemic also impeded public engagement with the bill, given restrictions on gatherings and the increased risk that COVID presented to those living with disabilities.
Legal scholar Isabel Grant argues that Bill C-7 is “legislated ableism”: “The state offering death as a solution to the suffering of disability for those not at the end of life is inherently ableist and based on the discriminatory premise that disability can be worse than death and, therefore, that death is a benefit for this group of Canadians.” 58 58 Grant, “Legislated Ableism,” 262. Gabrielle Peters, a disability writer and policy analyst, says, “Canada’s MAiD program didn’t invent discrimination against disabled people. It reified and built onto long-standing, deeply entrenched and entangled beliefs, customs, institutions, and conditions about and around disability and the construction of ‘other.’” 59 59 Peters, “Creating a Killable Class,” 209. Peters is also the co-founder of Disability Filibuster, whose opposition to C-7 was cited in footnote 57. Further, scholar Valentina Capurri suggests that a eugenics logic is at play, whereby an “understanding of what constitutes a life worth living encourages disabled and diseased individuals to conceive of their existence as worthless and to look at assisted dying as a possible solution.” 60 60 Capurri, “Canada’s Medical Assistance in Dying,” 55.
UN officials raised significant concerns about Bill C-7 and MAiD—specifically, the Special Rapporteur on the rights of persons with disabilities, the Independent Expert on the enjoyment of all human rights by older persons, and the Special Rapporteur on extreme poverty and human rights. In a 2021 letter addressed to the Canadian government, they expressed their concerns that Bill C-7 “risks furthering the devaluation of life with disability and reiterating the ableist stereotype that significant disability can be worse than death.” 61 61 Quinn, Mahler, and De Schutter, “Mandates of the Special Rapporteur on the Rights of Persons with Disabilities,” 6.
More recently, the UN Committee on the Rights of Persons with Disabilities reviewed Canada’s implementation of the UN Convention on the Rights of Persons with Disabilities and had harsh words to say about MAiD’s impact on Canadians with disabilities. The committee recommended, among other measures, the repeal of Track 2 and opposition to proposals for further MAiD expansion. 62 62 Committee on the Rights of Persons with Disabilities, “Convention on the Rights of Persons with Disabilities,” 7.
Discussion
How then should we understand the fact that persons with disabilities expressed overall support for MAiD under Tracks 1 and 2 in the fall 2024 ARI polling data, when such support is at odds with the opposition of a significant number of disability advocates and organizations? What could explain this difference?
While these data unfortunately do not allow us to answer this question definitively, previous polling data and other academic research suggest some possibilities that warrant further exploration.
First, the limitations of the sampling, discussed earlier, may be a factor. Broader samples of persons with disabilities are needed to better understand the views of this cohort in their full complexity.
Second, gaps in knowledge and misunderstandings about Canada’s MAiD law, as found in the Choi et al. and Tapp et al. studies, are likely at play. In other words, many Canadians living with disabilities may not understand how broad MAiD’s eligibility is or that they themselves may be eligible. Canadians living with disabilities, in line with the general population, likely support a much narrower MAiD eligibility—namely, MAiD as a last resort—rather than what is offered under the current law. Further, we do not know to what extent Canadians who support the law are aware of cases of MAiD driven by social suffering, or of the concerns that the MAiD Death Review Committee of Ontario has raised.
Finally and most significantly, given that those living with disabilities encounter deficiencies in healthcare, might there be a connection between receipt of inadequate care and support of MAiD? Does a struggle for care result in premature death becoming preferable to living? Again, we cannot make this conclusion based on the fall 2024 ARI data, but a 2023 ARI poll did find that respondents who were suffering from mental illness and said they had difficulties accessing mental health care were more likely to support MAiD for mental illness as a sole underlying condition, compared to the general population. 63 63 Angus Reid Institute, “Mental Health and MAID; Canadians who struggle to get help.”
This possibility is also suggested through anecdotal accounts of MAiD recipients who accessed MAiD not because of their disability but because of their struggles to receive assistance and care. As Sathya Dhara Kovac expressed in her obituary after her MAiD death in 2022, “Ultimately it was not a genetic disease [ALS] that took me out, it was a system. There are not enough supports and services promoting quality of life and Independence [sic] for those who are not healthy and able-bodied. . . . I could have had more time if I had more help.” 64 64 Kovac, “Sathya Dhara Kovac.”
MAiD’s Impact on Trust in Healthcare
Trust is critically important for physician-patient relationships and for the functioning of the healthcare system as a whole. Regardless of one’s views of the morality or acceptability of MAiD, its introduction into healthcare marks a striking departure from previously accepted norms and ethics in medicine, including the Hippocratic Oath’s to “do no harm” and the development of the palliative care approach, which, by definition, does not hasten death. This change implicates not only the broader posture of the state to citizens’ healthcare but also the individual and collective relationships between physicians, patients, and healthcare institutions. 65 65 Pedri, “Patient–Physician Relationship and MAID,” 387; Shariff and Gingerich, “Endgame.”
Persons with disabilities already, prior to MAiD, have had to fight against barriers to care and ableist assumptions about their quality of life, oftentimes having to advocate strenuously to receive basic care or relying on a loved one to advocate for them. The historical backdrop for Canadians living with disabilities includes not-too-distant memories of compulsory institutionalization of persons with disabilities and eugenic policies. 66 66 Reinders, Stainton, and Parmenter, “The Quiet Progress of the New Eugenics”; Frazee, “MAID Resistance in Canada.” For many of these Canadians, trust in healthcare institutions and professionals was already worn quite thin. 67 67 Peters, “Creating a Killable Class.” The introduction of MAiD intensifies these concerns.
Disability advocates and organizations have testified to their own efforts to respond to those who are seeking MAiD because of their circumstances and not their health condition or disability. As Catherine Frazee, disability scholar and former chief commissioner of the Ontario Human Rights Commission, articulated to a parliamentary committee, “We now spend every waking hour, every moment and resource not already spent on our own survival, throwing out lifelines to pull our disabled kinfolk back from the vortex that funnels them into the beckoning arms of Track 2 MAiD.” 68 68 Frazee, “Testimonial of Catherine Frazee,” 220.
The Doctor–Patient Relationship
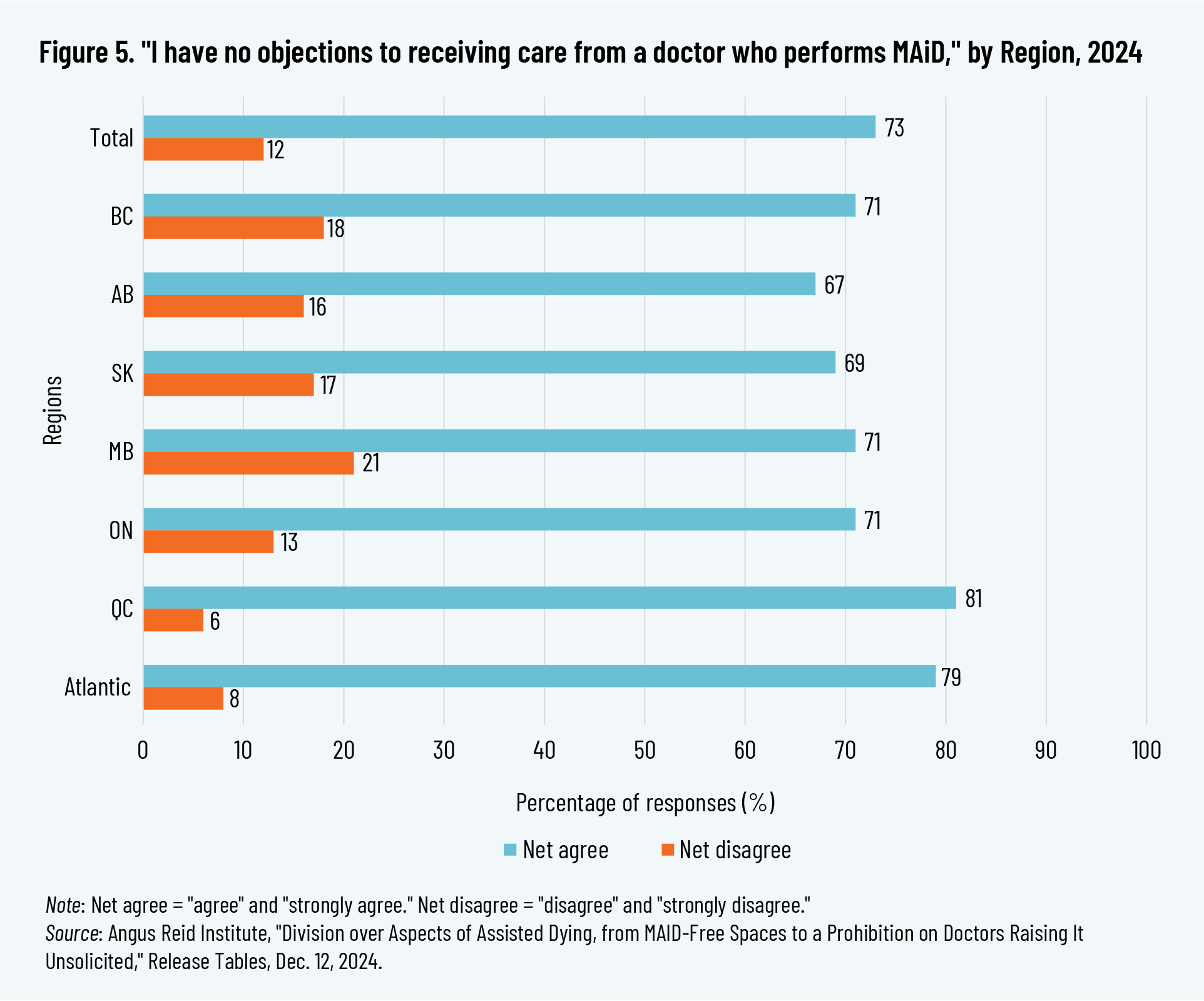
The fall 2024 ARI poll found that only a minority of Canadians (12 percent) expressed concern about receiving care from a doctor who also provides MAiD, while 73 percent expressed no concern. 69 69 Angus Reid Institute, “Division over Aspects of Assisted Dying,” 4. When considering these responses by province, these numbers vary significantly, as shown in figure 5.
Despite the general lack of concern on this matter, however, there are good reasons to question how MAiD may affect trust in physicians.
Comparing the massive growth of MAiD in Canada to the much lower uptake in California, Daryl Pullman points to the more direct role of providers in Canada as potentially having an influence on the higher rates, because even careful efforts on the part of the physician to explore the options “could be perceived as an endorsement of that option.” 70 70 Note that both jurisdictions legalized assisted dying in 2016 and have similarly-sized populations, although California allows only assisted suicide—and not euthanasia—and thus the physician’s role is much diminished compared to Canadian practice. Pullman, “Slowing the Slide,” 69.
This concern becomes more significant for Track 2 cases, in which the patient is not in fact dying. As Isabel Grant explains, the presentation of MAiD as “treatment”
permits medical professionals to offer MAiD to persons who are not otherwise seeking it, which may undermine a person’s trust in their doctor and send a signal that the physician has lost hope. This change in the relationship between doctors and persons with disabilities may deter people from either seeking medical support in their most vulnerable moments or from fully disclosing the extent of their suffering. 71 71 Grant, “Legislated Ableism,” 310–11.
Some international jurisdictions that have legalized assisted dying recognize the power dynamic inherent in the relationship between medical practitioners and patients and specifically prohibit practitioners from initiating discussions on assisted dying, as a “key safeguard.” Instead, patients must raise the issue first. 72 72 Parliament of New Zealand, The End of Life Choice Act 2019; Government of South Australia, SA Health, Voluntary Assisted Dying in South Australia Explained.
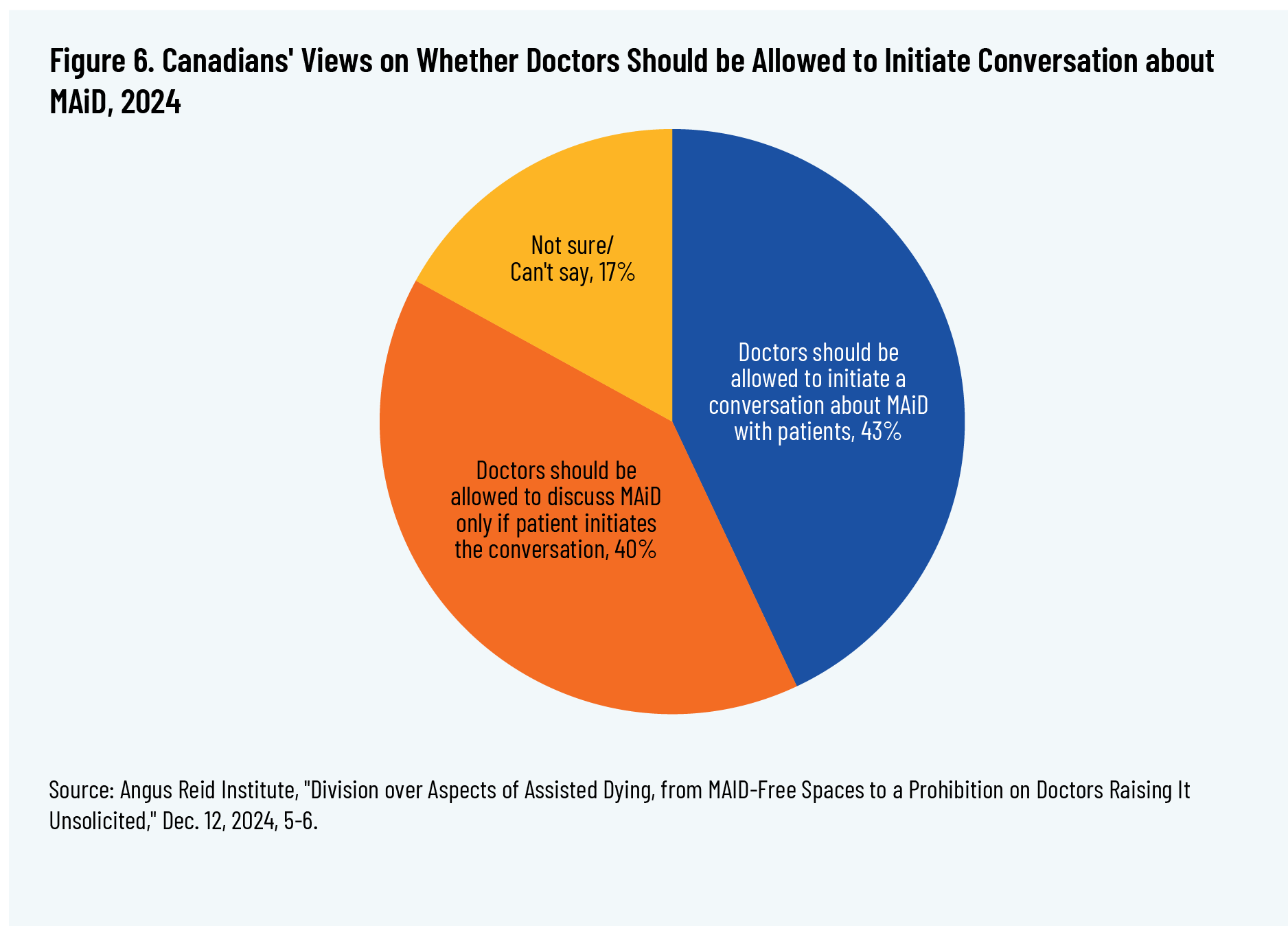
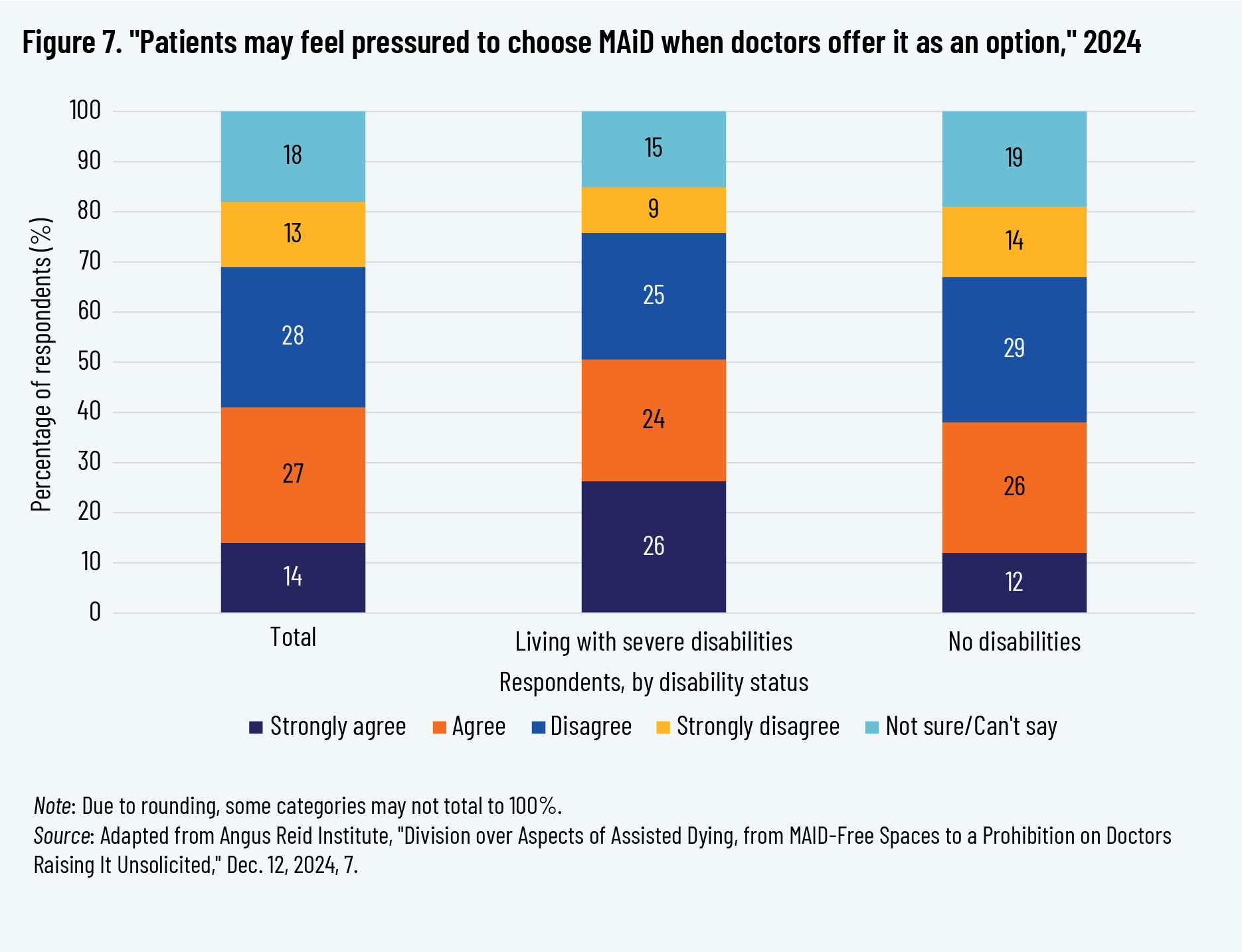
When asked in the ARI fall 2024 survey, Canadians were split on whether doctors should be prohibited from raising the subject of MAiD unsolicited, with 43 percent believing doctors should be allowed to mention it and 40 percent in favour of prohibiting it (17 percent responded “not sure/can’t say”). There was a similar split on whether raising MAiD unsolicited might affect patients’ decision-making: 41 percent agreed that “patients may feel pressured to choose MAID when doctors offer it as an option,” 41 percent disagreed, and 18 percent were unsure.
Importantly, this poll found that Canadians living with severe disabilities were more likely to agree that patients might feel pressured to choose MAiD when it is raised by their doctor, at 50 percent, compared to 38 percent of those with no disabilities. As depicted in figure 7, Canadians living with severe disabilities were much more likely to strongly agree (26 percent) than were all respondents as a whole (14 percent) and those with no disabilities (12 percent).
The mere possibility that raising MAiD unsolicited could result in pressure—even if unintended—should be taken very seriously, given that the Canadian law does not require patients to actually be provided with supports or alternatives. The physician’s duty is to offer alternatives, but simply offering alternatives such as disability supports may not be meaningful to a patient if they have long been struggling to access adequate care and the supports are not actually accessible.
MAiD-Free Spaces as Safe Spaces
Some healthcare facilities in Canada are unwilling to provide MAiD or participate in MAiD assessments. This has triggered debate and even lawsuits over the right of institutions to take these stances. 73 73 DeRosa, “Woman’s Family Sues B.C., Hospital Operator”; Canadian Press, “Catholic Church Challenging Quebec MAID Law.” Much of this debate has focused on the religious commitments of these institutions, such as Catholic hospitals, and their desire to exercise freedom of religion or of conscience, over against the desire of patients to receive MAiD in these facilities.
A dimension that is often overlooked in this debate is that some patients desire to receive healthcare specifically in facilities that do not provide MAiD. This is particularly relevant for communities that may be more vulnerable or for persons suffering from suicidal ideation. Gabrielle Peters addresses this issue from her perspective as a disabled woman, sharing her own challenging experience with hospitals and the healthcare system: “We should have the right to receive medical care in places and from people who do not contemplate or participate in killing disabled people as part of a care plan.” Peters also quotes Catherine Frazee, who stated, “On the question of religious hospitals, despite being a lesbian couple, Patricia and I would tolerate life-size crucifixes in the treatment room if it meant being safe from MAiD.” She goes on to describe Frazee’s words as representative of “a great many disabled people who fervently want safety from MAiD,” and who recognize that “the only MAiD-free spaces left are in faith-based facilities.” 74 74 Peters, “Reality, Not Religion, Is the Reason.”
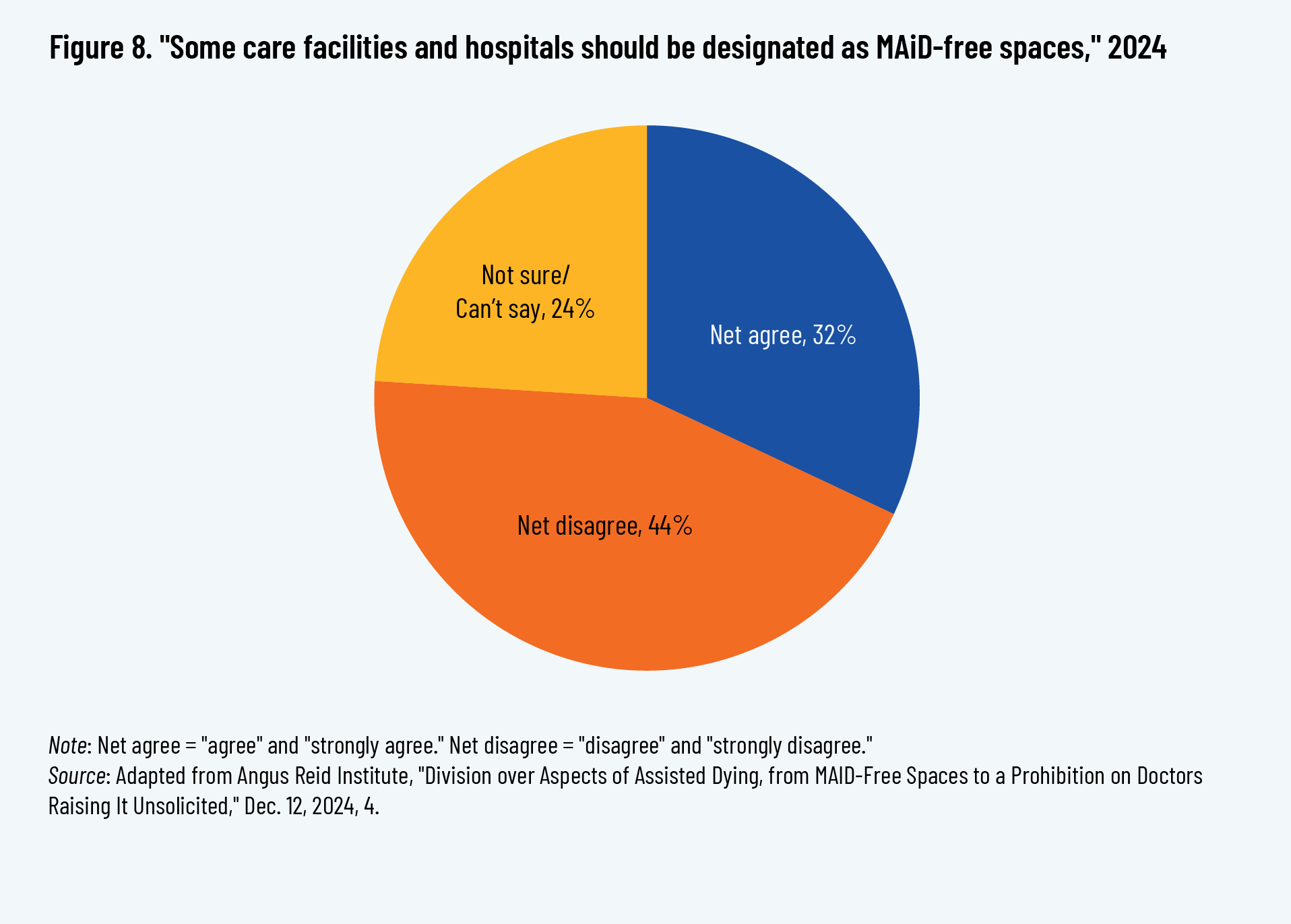
The fall 2024 ARI poll found that Canadians’ views were split on the desirability of MAiD-free spaces: 44 percent opposed designating some care facilities and hospitals as MAiD-free, and 32 percent were in favour. 75 75 Angus Reid Institute, “Division over Aspects of Assisted Dying,” 4. This result suggests that a significant proportion of Canadians want to have the option of a MAiD-free healthcare space or want that option to be available to others.
Less than a third of respondents said that institutions should be required to provide MAiD on site, whereas a slim majority agreed that MAiD-free institutions could, instead, transfer requesting patients to another facility where they could receive MAiD. 76 76 Angus Reid Institute, “Division over Aspects of Assisted Dying,” 3.
And, suggesting a heightened concern from Canadians with disabilities, those living with severe disabilities were more likely than respondents as a whole to support MAiD-free spaces (44 percent agreed, 38 percent disagreed), although the results still were generally split. Notably, however, those living with severe disabilities were twice as likely as other respondents to “strongly agree” with MAiD-free spaces (25 percent strongly agreed, compared to 12 percent of respondents overall). 77 77 Angus Reid Institute, “Division over Aspects of Assisted Dying,” 4.
Conclusion
Canadians’ views on MAiD continue to evolve, but majority opinion should not be the only metric by which policies and programs are judged. Minority views, particularly of those already living with significant vulnerabilities, should be taken seriously—especially when the program in question has resulted in the deaths of more than 76,000 Canadians since 2016. 78 78 Based on Health Canada reporting for 2016–2024. Health Canada, Sixth Annual Report, 10.
As this paper has reported, the ARI polling shows that most Canadians support the MAiD law, and their support has grown over time. Yet further research and other polling data demonstrate that Canadians do not understand what the MAiD law actually allows, and their support is in fact support for MAiD in exceptional or last-resort cases, which is incongruent with the actual law.
Further, a majority of Canadians are concerned that those struggling to access adequate care may as a result be influenced to opt for MAiD. And, as the ARI polling found, those living with disabilities face discrimination and barriers in care. These concerns are also found among the healthcare workers polled.
A broader consideration of research and disability voices on how inadequate care and ableism can influence MAiD decisions raises a host of red flags, heightened by the data available on MAiD in practice, including disturbing cases reported by the Ontario Coroner’s Office’s committee on MAiD.
And while Canadians are split on safeguards such as prohibiting physicians from raising MAiD unsolicited to patients or the ability of institutions to provide MAiD-free spaces, these measures warrant further consideration by policymakers in order to address the specific needs and concerns of Canadians with disabilities and others.
Significant work is needed to realize the goals expressed by the Canadian government in the preamble to its legislation that legalized euthanasia and assisted suicide:
Whereas it is important to affirm the inherent and equal value of every person’s life and to avoid encouraging negative perceptions of the quality of life of persons who are elderly, ill or disabled; Whereas vulnerable persons must be protected from being induced, in moments of weakness, to end their lives. 79 79 C-14, 2016, 1.
The importance of “a human rights-based approach to disability inclusion” that the government recognized in the preamble to the 2021 expansion of MAiD legislation 80 80 C-7, 2021, 1. demands that we take a harder look at the full context of disability in society, and recognize how facilitating the choice of MAiD for some individuals may in fact erode and damage the choices available to others, with lethal consequences.
References
Angus Reid Institute. “Disability & MAID: Three-in-Five Concerned Lack of Adequate Care May Push Vulnerable to Consider Assisted Dying.” November 21, 2024. https://angusreid.org/disability-maid-health-care-canada-medical-assisted-death/.
Angus Reid Institute. “Division over Aspects of Assisted Dying, from MAID-Free Spaces to a Prohibition on Doctors Raising It Unsolicited.” December 12, 2024. https://angusreid.org/assisted-dying-maid-free-space-canada/.
Angus Reid Institute. “MAID Spectrum HCW Tables.” 2024. https://angusreid.org/wp-content/uploads/2024/11/2024.11.19_MAID_spectrum_hcw_tables.pdf.
Angus Reid Institute. “Mental Health and MAID: Canadians Question Looming Changes to Canada’s Assisted-Death Law.” February 13, 2023. https://angusreid.org/assisted-dying-maid-mental-health/.
Angus Reid Institute. “Mental Health and MAID: Canadians Who Struggle to Get Help More Likely to Support Expanding Eligibility.” September 28, 2023. https://angusreid.org/mental-health-care-access-maid-mental-illness/.
ARCH Disability Law Centre. “Submission to Special Joint Committee on Medical Assistance in Dying.” November 16, 2023. https://archdisabilitylaw.ca/submission-to-special-joint-committee-on-medical-assistance-in-dying-2/.
Asada, Y., L. A. Campbell, M. Grignon, H. Hothi, T. Stainton, and S. Y. H. Kim. “Importance of Investigating Vulnerabilities in Health and Social Service Provision Among Requestors of Medical Assistance in Dying.” The Lancet Regional Health—Americas 35 (July 1, 2024). https://doi.org/10.1016/j.lana.2024.100810.
Ayers, T. “Cape Breton Woman Seeks MAID over Lengthy Workers’ Compensation Delays.” CBC News, August 22, 2023. https://www.cbc.ca/news/canada/nova-scotia/cape-breton-woman-seeks-medical-assistance-in-dying-over-wcb-delays-1.6942538.
Binkley, C.E., J.M. Reynolds, and A. Shuman. “From the Eyeball Test to the Algorithm—Quality of Life, Disability Status, and Clinical Decision Making in Surgery.” New England Journal of Medicine 387, no. 14 (2022): 1325–28. https://doi.org/10.1056/NEJMms2207408.
Bill C-7, An Act to Amend the Criminal Code (Medical Assistance in Dying). 43rd Parl, 2nd Sess. 2021. https://www.parl.ca/LegisInfo/en/bill/43-2/c-7.
Bill C-14, An Act to Amend the Criminal Code and to Make Related Amendments to Other Acts (Medical Assistance in Dying). 42nd Parl, 1st Sess. 2016. https://www.parl.ca/LegisInfo/en/bill/42-1/C-14.
Canadian Association of MAiD Assessors and Providers. “Clinical Practice Guideline: The Clinical Interpretation of ‘Reasonably Foreseeable.’” 2017. https://camapcanada.ca/wp-content/uploads/2022/02/Clinical-Interpretation-of-Reasonably-Foreseeable.pdf.
Canadian Press. “Catholic Church Challenging Quebec MAID Law in Court on Religious Freedom Grounds.” CTV News, February 6, 2024. https://www.ctvnews.ca/montreal/article/catholic-church-challenging-quebec-maid-law-in-court-on-religious-freedom-grounds/.
Capurri, V. “Canada’s Medical Assistance in Dying: Eugenics Under Another Name?” Canadian Journal of Disability Studies 14, no. 1 (2025): 45–70.
Carter v Canada (Attorney General). 2015. SCC 5. https://decisions.scc-csc.ca/scc-csc/scc-csc/en/item/14637/index.do?q=Carter.
CBC News. “B.C. Man with ALS Chooses Medically Assisted Death After Years of Struggling to Fund 24-Hour Care.” CBC News, August 13, 2019. https://www.cbc.ca/news/canada/british-columbia/als-bc-man-medically-assisted-death-1.5244731.
Choi, W.J.W., I.M. Astrachan, N. Sinaii, and S.Y.H. Kim. “When Medical Assistance in Dying Is Not a Last Resort Option: Survey of the Canadian Public.” BMJ Open 14, no. 6 (2024): e087736. https://doi.org/10.1136/bmjopen-2024-087736.
Coelho, R. “Disability and MAiD.” In Unravelling MAiD in Canada: Euthanasia and Assisted Suicide as Medical Care, edited by R. Coelho, K.S. Gaind, and T. Lemmens, 188–203. McGill-Queen’s University Press, 2025. https://www.mqup.ca/unravelling-maid-in-canada-products-9780228023692.php.
Committee on the Rights of Persons with Disabilities. “Convention on the Rights of Persons with Disabilities: Concluding Observations on the Combined Second and Third Periodic Reports of Canada.” United Nations, April 15, 2025. https://tbinternet.ohchr.org/_layouts/15/treatybodyexternal/Download.aspx?symbolno=CRPD%2FC%2FCAN%2FCO%2F2-3&Lang=en.
DeRosa, K. “Woman’s Family Sues B.C., Hospital Operator over MAID Policy.” CBC News, June 17, 2024. https://www.cbc.ca/news/canada/british-columbia/vancouver-woman-lawsuit-providence-health-maid-1.7237176.
De Vries McClintock, H.F., F.K. Barg, S.P. Katz, et al. “Health Care Experiences and Perceptions Among People with and Without Disabilities.” Disability and Health Journal 9, no. 1 (2016): 74–82. https://doi.org/10.1016/j.dhjo.2015.08.007.
Disability Filibuster. “About—Disability Filibuster.” https://disabilityfilibuster.ca/about/.
Favaro, A. “Police Investigating Medically-Assisted Death of BC Woman.” CTV News, April 26, 2022. https://web.archive.org/web/20240423112414/https://www.ctvnews.ca/health/police-investigating-medically-assisted-death-of-b-c-woman-1.5877288.
Favaro, A. “Woman with Chemical Sensitivities Chose Medically-Assisted Death After Failed Bid to Get Better Housing.” CTV News, April 13, 2022. https://www.ctvnews.ca/health/article/woman-with-chemical-sensitivities-chose-medically-assisted-death-after-failed-bid-to-get-better-housing/.
Frazee, C. “MAID Resistance in Canada: Sounding the Five-Minute Entreaty.” Canadian Journal of Disability Studies 13, no. 2 (2024): 1–175. https://cjds.uwaterloo.ca/index.php/cjds/article/view/1105.
Frazee, C. “Testimonial of Catherine Frazee.” Canadian Journal of Disability Studies 13, no. 2 (2024): 219–21. https://cjds.uwaterloo.ca/index.php/cjds/article/view/1117.
Gouvernment de Québec, Commission sur les soins de fin de vie. La Commission sur les soins de fin de vie. 2024. https://csfv.gouv.qc.ca/.
Government of South Australia, SA Health. Voluntary Assisted Dying in South Australia Explained. https://www.sahealth.sa.gov.au/wps/wcm/connect/public+content/sa+health+internet/services/community+and+specialised+services/voluntary+assisted+dying/explained/voluntary+assisted+dying+in+south+australia+explained.
Grant, I. “Legislated Ableism: Bill C-7 and the Rapid Expansion of Medical Assistance in Dying in Canada.” McGill Journal of Law and Health 15, no. 2 (2024): 259–335. https://commons.allard.ubc.ca/fac_pubs/739/.
Hachouch, Y., H. Akef, C. McDiarmid, S.M. Vachon, and D. Simionescu. “Barriers to Accessibility Related to Behaviours, Misconceptions or Assumptions: Findings from the 2022 Canadian Survey on Disability.” Statistics Canada, January 27, 2025. https://www150.statcan.gc.ca/n1/pub/89-654-x/89-654-x2025002-eng.htm.
Health Canada. Fifth Annual Report on Medical Assistance in Dying in Canada, 2023. December 2024. Updated February 1, 2025. https://www.canada.ca/en/health-canada/services/publications/health-system-services/annual-report-medical-assistance-dying-2023.html.
Health Canada. Sixth Annual Report on Medical Assistance in Dying in Canada, 2024. November 2025. https://www.canada.ca/en/health-canada/services/publications/health-system-services/annual-report-medical-assistance-dying-2024.html.
Iezzoni, L.I., S.R. Rao, J. Ressalam et al. “Physicians’ Perceptions of People with Disability and Their Health Care.” Health Affairs 40, no. 2 (2021): 297–306. https://doi.org/10.1377/hlthaff.2020.01452.
Inclusion Canada. “Bill C-7 Through a Disability Lens.” October 22, 2020. https://www.inclusioncanada.ca/resource?view=cc0ecf04-3edb-40cb-a56b-50d66eb06a0e.
Inclusion Canada. “Press Release: Disability Rights Coalition Challenges Discriminatory Sections of Canada’s Assisted Dying Law in Court.” September 26, 2024. https://inclusioncanada.ca/2024/09/27/press-release-disability-rights-coalition-challenges-discriminatory-sections-of-canadas-assisted-dying-law-in-court/.
Ipsos and Dying with Dignity Canada. “Support for Medical Assistance in Dying in Canada.” March 2025. https://www.dyingwithdignity.ca/wp-content/uploads/2025/04/DWDC_Ipsos_March2025_Final.pdf.
Janz, H. “MAID to Die by Medical and Systemic Ableism.” In Medical Assistance in Dying (MAID) in Canada: Key Multidisciplinary Perspectives, edited by J. Kotalik and D.W. Shannon, 299–308. International Library of Bioethics 104. Springer, 2023. https://doi.org/10.1007/978-3-031-30002-8.
Janz, H. “Plagued to Death by Ableism: What the COVID-19 Pandemic and the Expansion of Eligibility for MAID Reveal About the Lethal Dangers of Medical and Systemic Ableism in Canada.” Canadian Journal of Bioethics 6, no. 3–4 (2023): 137–41. https://doi.org/10.7202/1108012ar.
Kotalik, J. “Monitoring of MAID: Deficits of Transparency and Accountability.” In Medical Assistance in Dying (MAID) in Canada: Key Multidisciplinary Perspectives, edited by J. Kotalik and D.W. Shannon, 115–26. International Library of Bioethics 104. Springer, 2023. https://doi.org/10.1007/978-3-031-30002-8.
Kovac, S.D. “Sathya Dhara Kovac” (Obituary). Winnipeg Free Press, October 8, 2022. https://passages.winnipegfreepress.com/passage-details/id-311052/KOVAC_SATHYA.
Lagu, T., C. Haywood, K. Reimold, C. DeJong, R.W. Sterling, and L.I. Iezzoni. “‘I Am Not the Doctor for You’: Physicians’ Attitudes About Caring for People with Disabilities.” Health Affairs (Project Hope) 41, no. 10 (2022): 1387–95. https://doi.org/10.1377/hlthaff.2022.00475.
MacIvor, A. “A Halifax Woman Has Spent Years Fighting for Out-of-Province Care. Now She’s Ready to End Her Life.” CBC News, September 18, 2024. https://www.cbc.ca/news/canada/nova-scotia/jennifer-brady-lymphedema-nova-scotia-cancer-health-care-1.7322360.
Ministry of the Solicitor General, Office of the Chief Coroner for Ontario. MAiD Death Review Committee (MDRC) Report 2024 – 2: Complex Medical Conditions with Non-Reasonably Foreseeable Natural Deaths. 2024.
Ministry of the Solicitor General, Office of the Chief Coroner for Ontario. MAiD Death Review Committee Report 2024 – 3: Navigating Vulnerability in Non-Reasonably Foreseeable Natural Deaths. 2024.
Ministry of the Solicitor General, Office of the Chief Coroner for Ontario. MDRC Report 2024 – 4: Complex Same Day / Next Day Provisions. 2024.
Ministry of the Solicitor General, Office of the Chief Coroner for Ontario. Medical Assistance in Dying (MAiD): Marginalization Data Perspectives. 2024.
Parliament of New Zealand. The End of Life Choice Act 2019, Version as at 28 October 2021, Pub. L. No. Public Act 2019 No 67.https://www.legislation.govt.nz/act/public/2019/0067/latest/dlm7285905.html.
Pedri, L. “Patient–Physician Relationship and MAID: Trust and Autonomy.” In Medical Assistance in Dying (MAID) in Canada: Key Multidisciplinary Perspectives, edited by J. Kotalik and D.W. Shannon. International Library of Bioethics 104. Springer, 2023. https://doi.org/10.1007/978-3-031-30002-8.
Peters, G. “Creating a Killable Class and Manufacturing Selective Suicidality: Thoughts of a Past and Future Ironing Board.” In Unravelling MAiD in Canada: Euthanasia and Assisted Suicide as Medical Care, edited by R. Coelho, K.S. Gaind, and T. Lemmens, 204–76. McGill-Queen’s University Press, 2025. https://www.mqup.ca/unravelling-maid-in-canada-products-9780228023692.php.
Peters, G. “Reality, Not Religion, Is the Reason People Need MAiD-Free Health Care.” Policy Options, April 26, 2024. https://policyoptions.irpp.org/magazines/april-2024/maid-free-health-care/.
Pucchio, A.M.R., S. Stranges, and S. Ali. “Disability and Unmet Need for Health Care in Canada: Findings from the Canadian Community Health Survey.” Disability and Health Journal, April 30, 2025, 101846. https://doi.org/10.1016/j.dhjo.2025.101846.
Pullman, D. “Slowing the Slide Down the Slippery Slope of Medical Assistance in Dying: Mutual Learnings for Canada and the US.” American Journal of Bioethics 23, no. 11 (2023): 64–72. https://doi.org/10.1080/15265161.2023.2201190.
Quinn, G., C. Mahler, and O. De Schutter. “Mandates of the Special Rapporteur on the Rights of Persons with Disabilities; the Independent Expert on the Enjoyment of All Human Rights by Older Persons; and the Special Rapporteur on Extreme Poverty and Human Rights.” Geneva, Switzerland: Special, February 3, 2021. https://spcommreports.ohchr.org/TMResultsBase/DownLoadPublicCommunicationFile?gId=26002.
Raikin, A. “From Exceptional to Routine: The Rise of Euthanasia in Canada.” Cardus, 2024. https://www.cardus.ca/research/from-exceptional-to-routine/.
Raikin, A. “In Contrast to Carter: Assisted Dying’s Impact on Canadians with Disabilities.” Cardus, 2025. https://www.cardus.ca/research/health/reports/in-contrast-to-carter/.
Reinders, J., T. Stainton, and T.R. Parmenter. “The Quiet Progress of the New Eugenics. Ending the Lives of Persons with Intellectual and Developmental Disabilities for Reasons of Presumed Poor Quality of Life.” Journal of Policy and Practice in Intellectual Disabilities 16, no. 2 (2019): 99–112. https://doi.org/10.1111/jppi.12298.
Reynolds, J.M. “‘I’d Rather Be Dead than Disabled’—the Ableist Conflation and the Meanings of Disability.” Review of Communication 17, no. 3 (2017): 149–63. https://doi.org/10.1080/15358593.2017.1331255.
Rodriguez v British Columbia (Attorney General). 1993. SCC 3. https://decisions.scc-csc.ca/scc-csc/scc-csc/en/item/1054/index.do.
Saskatchewan Health Authority. “Accessing MAID in Saskatchewan.” https://www.saskhealthauthority.ca/your-health/conditions-illnesses-services-wellness/all-z/medical-assistance-dying/accessing-maid-saskatchewan.
Shakespeare, T., F. Ndagire, and Q.E. Seketi. “Triple Jeopardy: Disabled People and the COVID-19 Pandemic.” Lancet 397, no. 10282 (2021): 1331–33. https://doi.org/10.1016/S0140-6736(21)00625-5.
Shariff, M.J. “Carter v Canada: Exploring the Ebb and Flow of ‘Competing’ Societal Values Through Sections 7 and 1 of the Canadian Charter of Human Rights and Freedoms.” In Medical Assistance in Dying (MAID) in Canada: Key Multidisciplinary Perspectives, edited by J. Kotalik and D. W. Shannon, 25–53. International Library of Bioethics 104. Springer, 2023. https://doi.org/10.1007/978-3-031-30002-8.
Shariff, M.J., and M. Gingerich. “Endgame: Philosophical, Clinical and Legal Distinctions Between Palliative Care and Termination of Life.” Second Series Supreme Court Law Review 85 (June 1, 2018): 225–93.
Stainton, T. “Assisted Life Before Assisted Death: Disability Discomfort Regarding MAID.” In Medical Assistance in Dying (MAID) in Canada: Key Multidisciplinary Perspectives, edited by J. Kotalik and D.W. Shannon, 309–23. International Library of Bioethics 104. Springer, 2023. https://doi.org/10.1007/978-3-031-30002-8.
Stainton, T. “Disability, Vulnerability and Assisted Death: Commentary on Tuffrey-Wijne, Curfs, Finlay and Hollins.” BMC Medical Ethics 20, no. 1 (2019): 89. https://doi.org/10.1186/s12910-019-0426-2.
Tapp, D., G. Bravo, C. Filion, et al. “Individual Characteristics Influencing the General Population’s Level of Knowledge of End-of-Life Practices: A Cross-Sectional Study.” Palliative Care & Social Practice 19 (2025): 1–10. https://doi.org/10.1177/26323524241312922.
Watts, R. “Quadriplegic Quebec Man Chooses Assisted Dying after 4-Day ER Stay Leaves Horrific Bedsore.” CBC News, April 12, 2024. https://www.cbc.ca/news/canada/montreal/assisted-death-quadriplegic-quebec-man-er-bed-sore-1.7171209.
Watts, R. “Quebec Coroner Orders Public Inquiry into Assisted Death of Quadriplegic Man.” CBC News, June 25, 2024. https://www.cbc.ca/news/canada/montreal/coroner-s-inquiry-maid-quadriplegic-quebec-man-1.7245611.
Whitelaw, S., T. Lemmens, and H.G.C. Van Spall. “The Expansion of Medical Assistance in Dying in the COVID-19 Pandemic Era and Beyond: Implications for Vulnerable Canadians.” Canadian Journal of General Internal Medicine 17, no. 2 (2022): 17–21. https://doi.org/10.22374/cjgim.v17i2.586.