Table of Contents
Table of Contents
Key Points
- The Association of Christian Schools International and the School Counseling Mental Health Initiative at Denver Seminary surveyed Christian school educators in late 2024 on their perceptions of their students’ mental health and their own, and school practices and policies relating to mental health.
- About 80 percent of respondents rated the overall student mental health at their school as “good” or “excellent.” Some variation was observed across respondent role, grade level, and school type.
- Teachers gave slightly less favorable ratings than did other types of respondents, on average.
- Respondents at covenantal schools (which have a parental faith requirement) and elementary teachers across all school types rated students’ mental health more favorably, on average.
- Respondents at schools with cell phone policies in place rated students’ mental health more favorably, on average, versus schools with no policy in place.
- Respondents who reported that their schools paid attention to mental health gave more favorable assessments of student mental health, on average. Possible forms of attention included prioritizing mental health along with academic and spiritual development, showing compassion and understanding to those struggling with mental health challenges, openly acknowledging and advocating for the importance of mental health, providing information about mental health and support options, and being equipped as a school to address students’ mental health and wellness concerns.
- Respondents who reported integration of their school’s Christian mission with mental health approaches gave higher ratings of student mental health, on average. Possible forms of integration included school counselors or health professionals offering spiritually informed support options, religious service or devotional practices incorporating themes of mental health awareness and resilience, and providing programs that successfully connected students’ mental health needs with their spiritual mission.
- A strong relationship was observed between respondents’ assessment of their own well-being and their perceptions of student mental health. Those who reported feeling tired, worn out, physically exhausted, or emotionally exhausted were less likely to rate their students’ overall mental health as “good” or “excellent.” Respondents were also more likely to give a favorable rating of student mental health if they viewed their school’s faith-based approach as supporting their own mental health and wellness.
Introduction
Rates of anxiety, depression, and suicidality among school-aged children have been growing in recent years. 1 1 US Census Bureau, National Survey of Children’s Health; Kieling et al., “Worldwide Prevalence and Disability from Mental Disorders”; Centers for Disease Control and Prevention, Youth Risk Behavior Survey Data. Complete citations are provided for all sources at the end of this report. The Cardus Education Survey, a nationally representative survey of high school graduates aged 24 to 39, has found that adults from the four largest school sectors in the US (traditional public, Protestant Christian, Catholic, and non-sectarian private) all report similar levels of depression and anxiety, while homeschooled graduates report lower levels. 2 2 This finding remained even after controlling for a range of graduates’ background characteristics (e.g., family structure and religiosity, socioeconomic status), suggesting that this difference is likely attributable to type of schooling. Swaner, Cheng, and Eckert, “School-Sector Influence on Graduate Outcomes and Flourishing.” Although there are many factors that contribute to mental health, 3 3 Keyes, “Promoting and Protecting Mental Health as Flourishing.” the CES data prompt questions about the role of school-related experiences in the observed decline in youth mental health.
Educators themselves are also facing challenges. These include higher rates of burnout, which correlate with greater depression, anxiety, and overall stress. Several factors appear linked with teacher burnout, including aspects of the workplace that are logistical (e.g., class size, staffing levels) and relational (e.g., level of support from supervisors). Importantly, however, educator mental health appears to be linked with the mental health and well-being of students, suggesting that mental health concerns in schools are not solely an individual issue but rather reflect the interconnectedness of individuals and groups within the school ecosystem. 4 4 Agyapong et al., “Stress, Burnout, Anxiety and Depression Among Teachers”; Shen et al., “The Relationship Between Teacher Burnout and Student Motivation.”
When it comes to research on the influence of schools on student mental health, the findings vary. Some studies have shown that students’ experiences of connectedness at school are positively associated with their mental health. 5 5 McNeely and Falci, “School Connectedness and the Transition.” The influence of technology, including smartphone use, has received growing attention in schools because of connections between such use and declining youth mental health. 6 6 Haidt and Pratt, The Anxious Generation. As for school-based interventions, some evidence suggests that promoting mental health and using preventative approaches (e.g., community-wide education) can positively affect the entire school community, as can mental health interventions (e.g., individual and group counseling). 7 7 Townsend et al., “The Association of School Climate, Depression Literacy, and Mental Health Stigma.” At the same time, some studies have found that specific mental health treatment approaches in schools do not seem to result in better mental health outcomes, and in some cases, the outcomes were poorer. 8 8 Foulkes and Stringaris, “Do No Harm”; Harvey, White, Hunt, and Abbott, “Investigating the Efficacy of a Dialectical Behaviour Therapy-Based Universal Intervention.”
While these and many other factors can contribute to the prevalence of mental health concerns in schools, there are also realities unique to school type. As a sector, Christian schools in the US have not historically emphasized mental health support and education, focusing rather on spiritual and character development. 9 9 Wilson et al., “Student Mental Health Support in Private Christian Schools.” Fewer financial resources (as compared with those available to public school districts) may also contribute to the lack of systemic support for mental health reported by Christian school educators (such as lower numbers of school-employed mental health professionals). 10 10 Association of Christian Schools International, 2019–2020 Tuition & Salary Survey Member Report. There is also limited research investigating the mental health of US Christian school students and educators, as compared with the mental health of those groups in US public schools. 11 11 Thorton and Miller, “Mental Health and Well-Being in Faith-Based Schools.” At the same time, better mental health and well-being might be expected among Christian school students and educators, given that communal religious participation is correlated with greater levels of happiness and life satisfaction, mental health and physical health, meaning and purpose, and close social relationships. 12 12 VanderWeele, “Religious Communities and Human Flourishing.”
To better understand the current reality of student and educator mental health in Christian schools, the Association of Christian Schools International (ACSI) and the School Counseling Mental Health Initiative at Denver Seminary fielded an electronic survey in October 2024 to Christian school educators (leaders and teachers) employed at ACSI member schools in the US. ACSI is the largest Protestant Christian school association, with close to 5,500 member schools around the world, 2,300 of which are in the US. ACSI member schools are diverse in terms of school size (enrollment), structure (independent or church-sponsored), admissions policy (covenantal—requiring parental assent to a statement of faith and/or church attendance, or missional—not having that requirement), and urbanicity.
The results of the survey provide insight into the perceptions of Christian school educators in the US regarding their students’ mental health, school practices and culture when it comes to mental health, and their own well-being. This report shares key insights from the survey and concludes with a discussion of the results and their implications for Christian schools.
Methodology
The electronic survey on mental health was fielded in October 2024 for four weeks. An invitation to participate was emailed to all heads of school, administrators, and teachers working at ACSI member schools in the US, totaling over 10,000 individual invitations. 13 13 Respondents could select “head of school/superintendent,” “administrator (principals, vice principals, curriculum coordinator, etc.),” or “teacher” to identify their role in their school. A total of 1,344 individuals responded to the survey, for a response rate of about 13 percent. Of those, over 90 percent finished the survey (for this report, only these 1,277 surveys were analyzed). All results in this report are descriptive of this sample of survey respondents.
In addition to asking respondents demographic questions and about their school’s characteristics, the survey asked about respondents’ perceptions of mental health at their schools and the severity and types of mental health challenges they thought their students faced. The survey also asked about mental health-related support, resources, and policies at their schools. Finally, some questions asked for respondents’ views about the level of integration of religious faith with mental health at their schools, as well as their own mental health.
Respondent Demographics and School Characteristics
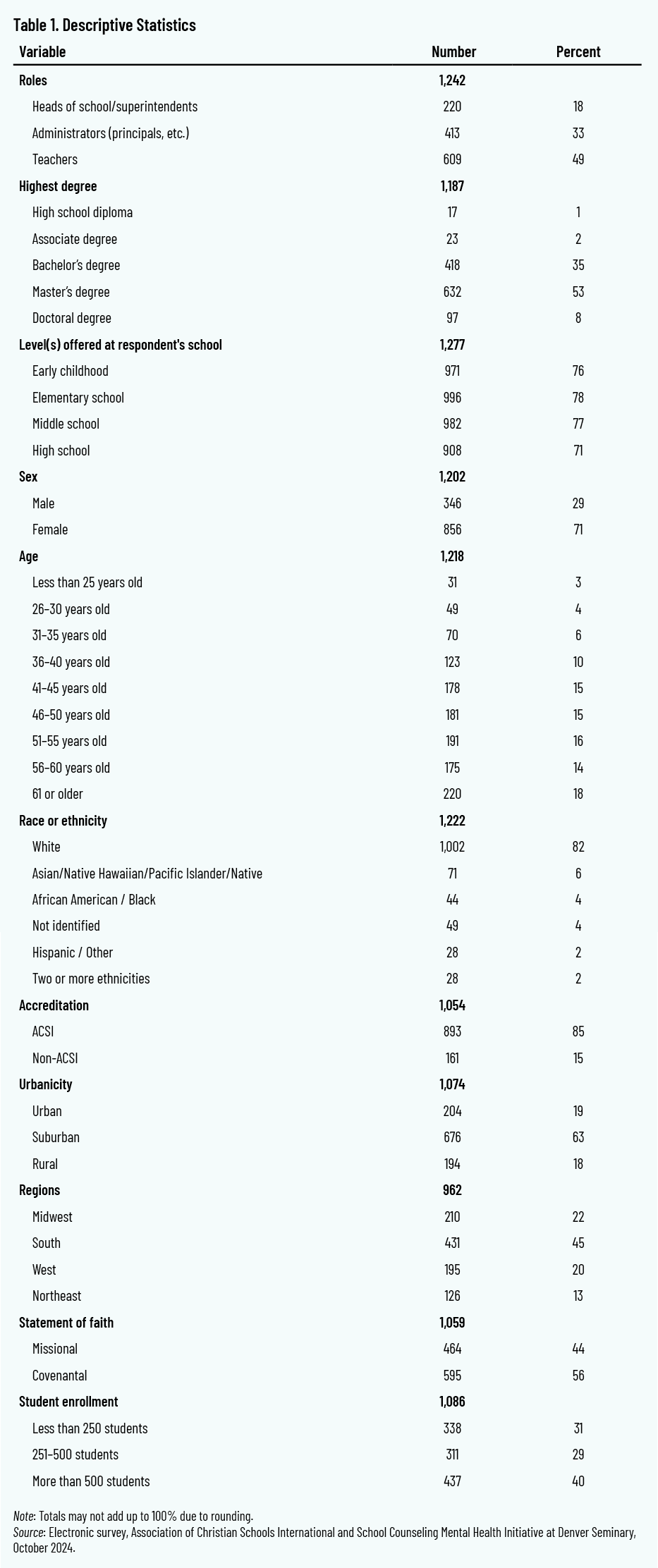
A majority of respondents were female (71 percent), and 45 percent were aged 41 to 55. About 18 percent of the respondents were heads of school or superintendents, 33 percent were administrators, and 49 percent were teachers. Over half of the respondents reported their highest degree as a master’s (53 percent) followed by those reporting a bachelor’s as their highest degree (35 percent). Respondents were primarily White (82 percent), followed by Asian American (6 percent), African American/Black (4 percent), and Latino/Hispanic (2 percent), with an additional 4 percent not identified.
As for school characteristics, 63 percent of respondents were at suburban schools, followed by 19 percent at urban schools and 18 percent at rural schools. In terms of geographic location, 45 percent of respondents were located in the South, 22 percent in the Midwest, 20 percent in the West, and the remaining 13 percent in the Northeast. In addition, 56 percent of respondents said they were at covenantal schools (i.e., schools that require parents to be active members of a church and/or to sign a statement of faith), while 44 percent were at missional schools (where no such requirement is in place). About 31 percent of respondents were employed at small schools (less than 250 students), 29 percent from medium-sized schools (251–500 students), and 40 percent at large schools (more than 500 students).
All of these proportions are roughly representative of ACSI schools in the US as a whole. The only exception was the percentage of respondents who said they worked at an ACSI-accredited school, which was higher in the sample (at 85 percent) than in ACSI membership.
Data Analysis
Two approaches were used to analyze the data, in keeping with prior research that ACSI and Cardus have conducted on Christian schools. 14 14 See Swaner and Djita, “Navigating AI in Christian Schools.” First, the report presents descriptive analyses (without controlling for respondents’ demographic background), with the goal of providing a baseline description of the data. This approach used standard statistical tests to determine whether a relationship exists between two variables. 15 15 Specifically, the analysis used the Chi-square test of independence.
The second approach used more in-depth statistical analysis to control for respondents’ demographic background (sex, highest degree obtained, and race/ethnicity) and school characteristics (school size, admissions policy, levels of education offered, accreditation status, urbanicity, and ACSI regional division). 16 16 Specifically, the analysis used multivariate regressions to control for the variables listed. The only exception is for analyses related to cell phone policies: instead of trying to separate the effects of phone policies from other factors, analysis of cell phone policies used unadjusted percentages to keep the results clear, easy to understand, and free from unnecessary statistical complexity. For teacher responses, the same variables were controlled but the grade levels taught were added. This means that the findings are more likely to be due to the variable being examined than to respondents’ demographic background and school characteristics.
The methodology for this study carries at least three limitations. First, the respondents may not be representative of the whole population of ACSI educators. Second, this approach cannot provide cause-and-effect (causal) data but instead enables observations of potential relationships (correlations) between variables. And third, the survey asked the respondents about their perceptions about their students, schools, and themselves, which is not the same as surveying students about their own perceptions or collecting data using objective measures of student mental health (e.g., mental health diagnoses by qualified professionals). 17 17 Educator perceptions were used in this study because collecting student self-reports of mental health, as well as official mental health data from schools, is both sensitive and difficult; this is because minors are involved and strict legal and privacy protections limit what data can be gathered, shared, and stored. While these limitations of the research design should be kept in mind when making inferences from the findings, the respondents’ perceptions are nonetheless helpful in making broad observations about mental health in Christian schools.
Key Findings
The survey examined educators’ perceptions of overall student mental health within their schools. Data analysis explored whether these perceptions varied according to:
- educator demographic background and school characteristics
- actions that the school has taken to support student mental health
- integration of Christian mission in school approaches to mental health
- school policies on student cell phone use
- educators’ own mental health and well-being
This section of the report presents the findings related to each of these, disaggregated by respondent group (heads of school, administrators, and teachers).
Overall Student Mental Health
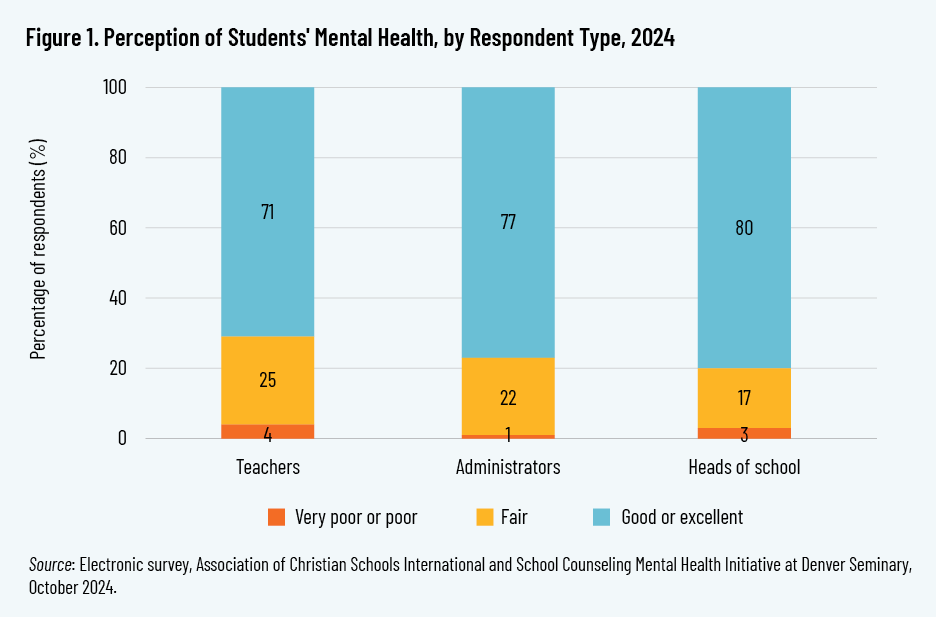
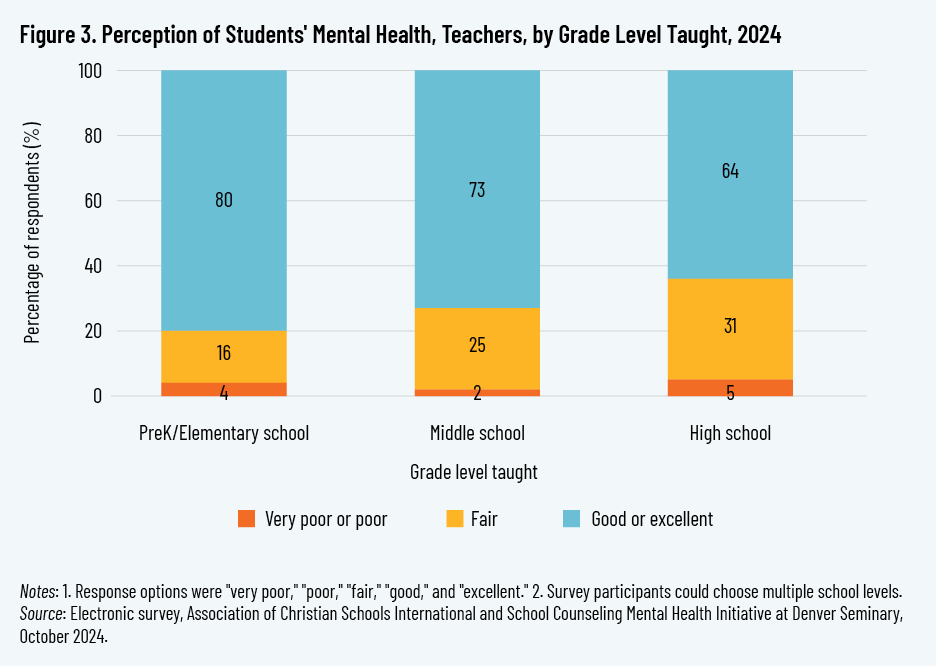
To gauge their perceptions of student mental health, respondents were asked, “How would you rate the overall mental health of students at your school?” Response options were “very poor,” “poor,” “fair,” “good,” and “excellent.” Perceptions of overall student mental health were mostly “good” or “excellent” across all respondent groups. Some differences existed between respondent groups, however. The percentages of “good” or “excellent” responses were highest among heads of school (80 percent) and lowest among teachers (71 percent), with administrators’ percentage closer to that of heads of school (at 77 percent). Thus, a greater percentage of teachers—who typically have the most direct and frequent contact with students—selected a lower level response than both heads of school and administrators.
In addition to respondent role, the study’s analysis also explored whether there were differences in perceptions of student mental health based on the characteristics of respondents’ schools—specifically, school size, admissions policy, and levels of education offered. The data show that school size is not correlated with respondents’ perceptions of overall student mental health.
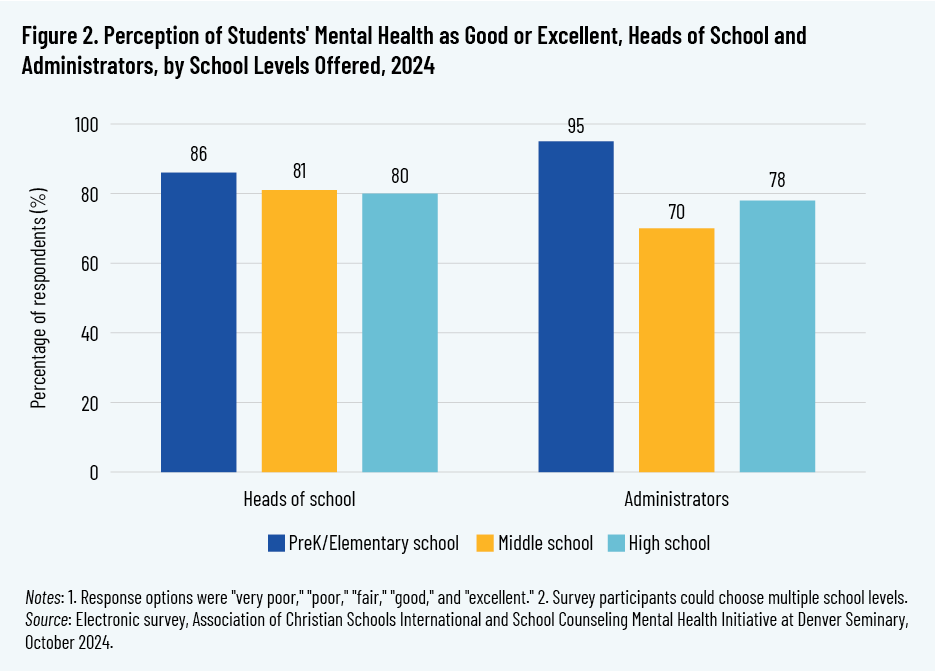
However, levels of education offered at respondents’ schools (pre-K/elementary, middle school, high school) were correlated with differences in responses. 18 18 Although classifications may differ slightly across some schools, for the purpose of this study, pre-K is defined as early childhood, preschool, and pre-kindergarten classes; elementary as kindergarten and first through fifth grade; middle school as sixth through eighth grade; and high school as ninth through twelfth grade. Heads of school and administrators at schools that offered only lower grades (pre-K and elementary) were more likely to rate their students’ mental health as “good” or “excellent,” as compared with their middle or high school counterparts. Similarly, teachers who taught pre-K and elementary grades had a higher assessment of overall student mental health, on average, than did teachers who taught middle or high school grades.
Differences in how respondents perceived student mental health also emerged based on their school admissions policy. Respondents were asked, “Does your school require parents to be active members of church and/or to sign a statement of faith upon the admission of their children to the school?” Those who answered “yes” were categorized as working in covenantal schools, while those who answered “no” were categorized as working in missional schools. 19 19 The terms “covenantal” and “missional” are commonly used within the Christian school sector in the US to describe these admission policies. However, other terms are sometimes used. Analyses showed that heads of school and administrators at covenantal schools were more likely to rate overall student mental health as “good” or “excellent.” Responses of teachers at these two types of schools, however, did not differ significantly.
School Actions to Support Student Mental Health
Respondents were asked to rate their level of agreement with the following statements concerning actions that their schools might be taking with the intent of supporting students’ mental health:
- Our school generally prioritizes mental health and wellness alongside academic and spiritual development.
- The school community shows compassion and understanding toward individuals facing mental health and wellness challenges.
- School leadership openly acknowledge and advocate for the importance of mental health within the school community.
- Our school regularly provides information about mental health and wellness resources and support options.
- School announcements, assemblies, or curriculum incorporate information about mental health awareness and wellness.
- Our school is equipped to address situations involving students struggling with mental health and wellness concerns.
Response options for each statement were “strongly agree,” “agree,” “neutral,” “disagree,” and “strongly disagree.” For analysis, the responses were later collapsed into two categories: “agree” (“strongly agree,” “agree,” and “neutral”) and “disagree” (“disagree” and “strongly disagree”). 20 20 The “neutral” option was placed in the “agree” category to capture a broader range of non-negative sentiment toward the statement, as neutrality often reflects an absence of disagreement rather than active opposition. For each statement, respondents in the “agree” group were more likely to rate the overall student mental health at their school as “good” or “excellent,” compared with respondents in the “disagree” group (by a difference as high as 35 percentage points). This finding was constant across the three respondent groups (heads of school, administrators, and teachers) even after controlling for respondents’ demographic background and school characteristics.
Integration of Christian Mission
The survey asked respondents to rate their agreement with the following statements, which relate to the integration of their schools’ Christian mission with its approaches to mental health:
- My school integrates faith and spiritual guidance into its approach to supporting mental health and wellness.
- School counselors or health professionals in this school offer faith-based or spiritually informed support options.
- Religious service or devotional practices incorporate themes of mental health awareness and resilience.
- My school provides programs that successfully connect students’ mental health needs with their spiritual foundation.
The response options and subsequent groupings were the same as in the preceding section. For each statement, respondents in the “agree” group were more likely to rate students’ overall mental health as “good” or “excellent,” compared to respondents in the “disagree” group (by a difference as high as 45 percentage points). This finding was constant across the three respondent groups (heads of school, administrators, and teachers) even after controlling for respondents’ demographic background and school characteristics.
Cell Phone Policies
Respondents were asked whether their school had a cell phone policy or restricted students’ cell phone use. Almost all who rated their students’ mental health as “good” or “excellent” affirmed that their school did this (98 percent).
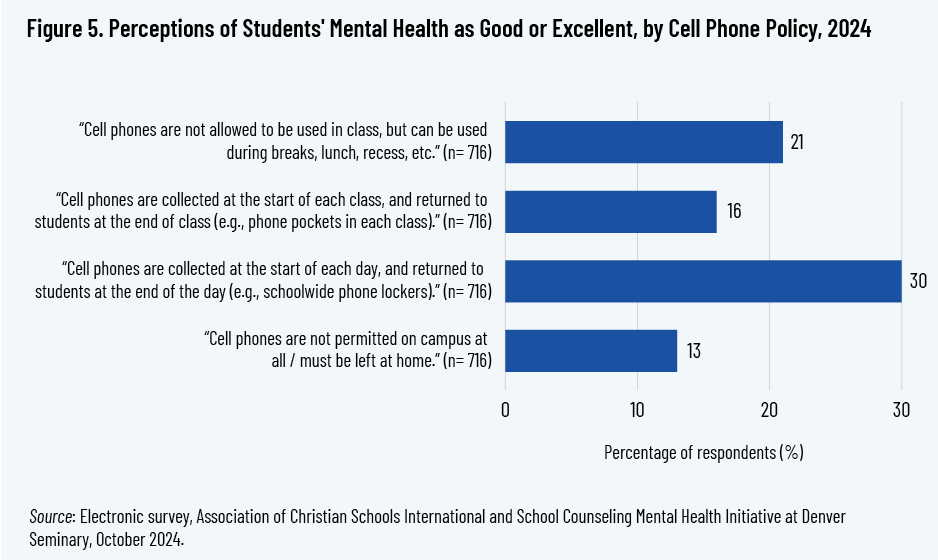
Respondents who indicated that their school had a cell phone policy in place or restricted cell phone use were then asked to respond “yes” or “no” to each of the following statements:
- Cell phones are not allowed to be used in class but can be used during breaks, lunch, recess, etc.
- Cell phones are collected at the start of each class and returned to students at the end of class (e.g., phone pockets in each class).
- Cell phones are collected at the start of each day and returned to students at the end of the day (e.g., schoolwide phone lockers).
- Cell phones are not permitted on campus at all/must be left at home.
The response option that was most highly correlated with respondents’ perception of “good” or “excellent” student mental health was collecting phones at the start of each day and returning them at the end.
Educator Well-Being
The survey asked respondents to rate their level of agreement with each of the following statements related to their own well-being:
- I feel tired.
- I feel worn out.
- I am physically exhausted.
- I am emotionally exhausted.
- I feel weak and susceptible to illness.
- I think “I can’t take it anymore.”
Here again, the response options and subsequent groupings were as described in the preceding sections. For each of these statements, respondents in the “agree” group were less likely to rate students’ overall mental health as “good” or “excellent,” compared with respondents in the “disagree” group (by a difference as high as 27 percentage points). In other words, respondents who felt worse about their own well-being were more likely to perceive their students’ overall mental health as poorer. This finding was constant across the three respondent groups even after controlling for respondents’ demographic background and school characteristics.
Discussion
This study explored Christian school educators’ perceptions of students’ mental health and their own mental health, school practices relating to mental health, and their school’s cell phone policy. While the study does not include student responses or objective mental health data, the educators’ perceptions still offer several key insights for understanding the state of mental health in Christian schools.
First, this study provides a window into Christian school educators’ view of overall student mental health, and how views vary in relation to respondents’ demographic background and school characteristics. The great majority of respondents rated student mental health at their schools as “good” or “excellent,” which is an encouraging finding. Yet this finding varies across role and grade level. Teachers, who interact with students most closely, were least likely of the three groups of respondents to rate student mental health at their schools as “good” or “excellent.” Middle and high school teachers were less likely to rate student mental health at their schools as “good” or “excellent” than were pre-K and elementary teachers. And heads of school and administrators at missional schools were less likely to rate student mental health as “good” or “excellent” than were their peers at covenantal schools. Teachers at missional schools were similar to teachers at covenantal schools in their average rating of student mental health.
Correlations do not allow for conclusions about cause and effect, but each of these findings might be expected. First, teachers are “front line” engagers with students, while heads of school and administrators are more removed; this may give teachers a greater awareness of students’ daily struggles. Second, students in middle and high school are older and often dealing with greater academic and social pressures than younger students and thus may face more, or more severe, mental health challenges; it might therefore be expected that teachers in the middle and high school grades would perceive lower levels of student mental health than their peers who teach the younger grades. And third, student mental health might be slightly lower at missional than at covenantal schools due to the positive correlation that is known to exist between religious engagement and well-being. 21 21 VanderWeele, “Religious Communities and Human Flourishing.” This study found mixed support for this conclusion, as heads of school and administrators at covenantal schools rated student mental health higher, on average, than did their peers at missional schools, but teachers at the two types of schools rated their students’ mental health at similar levels.
Across all analyses, institutional attention to mental health was associated with higher perceived student well-being. Possible school actions included prioritizing mental health and wellness along with academic and spiritual development; showing compassion and understanding to those struggling with mental health challenges; leaders openly acknowledging and advocating for the importance of mental health; providing information about mental health and support options and including that information in school announcements, assemblies, and curricula; and being equipped as a school to address students’ mental health and wellness concerns. Additionally, educators at schools with cell phone policies were much more likely to report higher perceptions of overall student mental health.
It should be noted that the study did not ask respondents about specific wellness programs or treatment options that their schools might arrange for individual students, but rather asked about broad, whole-school actions their schools might be engaged in to address student mental health. The study findings suggest that Christian schools can positively address student mental health through these broader actions, like providing an education that addresses the whole person, showing compassion and advocating for those who are struggling, and sharing information and resources to support students’ well-being.
In terms of educator well-being, because the study did not use a representative sample, it is not possible to estimate the perceived well-being of educators at Christian schools as a population. However, for the educators surveyed, a strong relationship was observed between their perceptions of their own well-being and that of their students. When educators reported one or more signs of stress and strain—such as feeling tired, worn out, physically exhausted, emotionally exhausted, weak and susceptible to illness, or thinking “I can’t take it anymore”—they rated their students’ mental health lower, on average. These findings suggest that Christian schools should consider the well-being of both students and staff as part of any mental health approach. Schools may wish to consider positive actions such as investment in staff support systems and realistic workloads; to the degree that these or similar actions benefit educator well-being, they can in turn help educators to model well-being to their students.
Finally, respondents who reported integration of their school’s Christian mission with mental health approaches at their school rated their students’ mental health higher, on average. This finding suggests that schools should consider taking a holistic approach to student mental health—one that recognizes human beings as whole persons and that integrates spiritual and psychological dimensions. This finding is aligned with the theological perspective that undergirds Christian schools: educators are entrusted not only with their students’ intellectual growth but also with their overall development as persons. Theologian and Christian educator Neal Plantinga describes the aim of this development and growth in terms of the Hebrew word shalom: “In the Bible, shalom means universal flourishing, wholeness, and delight—a rich state of affairs in which natural needs are satisfied and natural gifts fruitfully employed, all under the arch of God’s love.” 22 22 Plantinga, Engaging God’s World, 15. Schools that connect mental health with their Christian mission are thus not adding a secular layer to faith-based education but rather deepening their witness to the holistic redemption that Scripture envisions for human life.
Future Directions
While this study generated several insights for Christian schools, important limitations must be acknowledged. The study relies on educator perceptions, which may not be as reliable as direct observations of student mental health. To address this limitation, future research could incorporate objective data on student mental health, student self-assessment, parents’ perceptions, and longitudinal tracking of the outcomes of specific approaches. Future research could also examine how different theological traditions inform how Christian schools frame and respond to mental health challenges.
Finally, it would be valuable to investigate the mechanisms by which faith integration contributes to better perceived mental health, both for students and educators. For example, does faith integration benefit mental health through increased social support, greater meaning-making, or a shared moral vocabulary around suffering and hope? Qualitative and mixed-method studies could illuminate how educators in Christian schools articulate and embody this integration in daily school life.
This study underscores that Christian schools have the opportunity and responsibility to cultivate environments in which student and educator well-being is valued, prioritized, and supported. At the same time, a school’s Christian mission can be beneficial to the mental health and well-being of both students and educators. This goes beyond simply offering support services or restricting cell phone use, to forming communities grounded in love of God and neighbor and in which emotional and spiritual well-being are nurtured together.
References
Agyapong, B., G. Obuobi-Donkor, L. Burback, and Y. Wei. “Stress, Burnout, Anxiety and Depression Among Teachers: A Scoping Review.” International Journal of Environmental Research and Public Health 19, no. 17 (2022): Article 10706. https://doi.org/10.3390/ijerph191710706.
Association of Christian Schools International. 2019–2020 Tuition & Salary Survey Member Report. ACSI, 2020. https://www.acsi.org/docs/default-source/website-publishing/research/acsi_tuitionsalary_report-2019-2020.pdf?sfvrsn=9a654d6_2.
Centers for Disease Control and Prevention. Youth Risk Behavior Survey Data. CDC, 2023. https://www.cdc.gov/yrbs/dstr/index.html.
Cheng, A., M.H. Lee, and R. Djita. “A Cross-Sectional Analysis of the Relationship Between Sabbath Practices and US, Canadian, Indonesian, and Paraguayan Teachers’ Burnout.” Journal of Religion and Health 62 (2023):1090–113. https://doi.org/10.1007/s10943-022-01647-w.
DeLuca, J.S. “Conceptualizing Adolescent Mental Illness Stigma: Youth Stigma Development and Stigma Reduction Programs.” Adolescent Research Review 5 (2020): 153–71. https://doi.org/10.1007/s40894-018-0106-3.
Foulkes, L., and A. Stringaris, “Do No Harm: Can School Mental Health Interventions Cause Iatrogenic Harm?” BJPsych Bulletin 47, no. 5 (2023): 267–69. https://doi.org/10.1192/bjb.2023.9.
Haidt, J., and S. Pratt. The Anxious Generation: How the Great Rewiring of Childhood Is Causing an Epidemic of Mental Illness. Penguin Random House, 2024.
Harvey, L.J., F.A. White, C. Hunt, and M. Abbott. “Investigating the Efficacy of a Dialectical Behaviour Therapy-Based Universal Intervention on Adolescent Social and Emotional Well-being Outcomes,” Behaviour Research and Therapy 169 (2023): 104408. https://doi.org/10.1016/j.brat.2023.104408.
Keyes, C.L.M. “Promoting and Protecting Mental Health as Flourishing: A Complementary Strategy for Improving National Mental Health.” American Psychologist 62, no. 2 (2007): 95–108. https://doi.org/10.1037/0003-066X.62.2.95.
Kieling, C., C. Buchweitz, A. Caye et al. “Worldwide Prevalence and Disability from Mental Disorders Across Childhood and Adolescence: Evidence from the Global Burden of Disease Study.” JAMA Psychiatry 81, no. 4 (2024): 347–56. https://doi.org/10.1001/jamapsychiatry.2023.5051.
Lever, N., E. Mathis, and A. Mayworm. “School Mental Health Is Not Just for Students: Why Teacher and School Staff Wellness Matter.” Report on Emotional and Behavioral Disorders in Youth 17, no. 1 (2019). https://pmc.ncbi.nlm.nih.gov/articles/PMC6350815/.
Ma, K.K.Y., J.K. Anderson, and A.M. Burn. “Review: School-Based Interventions to Improve Mental Health Literacy and Reduce Mental Health Stigma—A Systematic Review.” Child and Adolescent Mental Health 28, no. 2 (2023): 230–40. https://doi.org/10.1111/camh.12543.
McNeely, C., and C. Falci. “School Connectedness and the Transition Into and Out of Health-Risk Behavior Among Adolescents: A Comparison of Social Belonging and Teacher Support.” Journal of School Health 74, no. 7 (2004): 284–92. https://doi.org/10.1111/j.1746-1561.2004.tb08285.x.
Milin, R., S. Kutcher, S.P. Lewis et al. “Impact of a Mental Health Curriculum on Knowledge and Stigma Among High School Students: A Randomized Controlled Trial.” Journal of the American Academy of Child & Adolescent Psychiatry 55, no. 5 (2016): 383–91. https://doi.org/10.1016/j.jaac.2016.02.018.
Plantinga Jr., C. Engaging God’s World: A Christian Vision of Faith, Learning, and Living. Eerdmans, 2002.
Radez, J., T. Reardon, C. Creswell, P.J. Lawrence, G. Evdoka-Burton, and P. Waite. “Why Do Children and Adolescents (Not) Seek and Access Professional Help for Their Mental Health Problems? A Systematic Review of Quantitative and Qualitative Studies.” European Child & Adolescent Psychiatry 30 (2021): 183–211. https://doi.org/10.1007/s00787-019-01469-4.
Shen, B., N. McCaughtry, J. Martin, A. Garn, N. Kulik, and M. Fahlman. “The Relationship Between Teacher Burnout and Student Motivation.” British Journal of Educational Psychology 85, no. 4 (2015): 519–32. https://doi.org/10.1111/bjep.12089.
Swaner, L.E., A. Cheng, and J. Eckert. “School-Sector Influence on Graduate Outcomes and Flourishing: Findings from the 2023 Cardus Education Survey.” Cardus, 2024. https://www.cardus.ca/research/education/reports/school-sector-influence-on-graduate-outcomes-and-flourishing/.
Swaner, L.E., and R. Djita. “Navigating AI in Christian Schools.” Cardus, 2024. https://www.cardus.ca/research/education/reports/navigating-ai-in-christian-schools/.
Swartz, K.L., E.A. Kastelic, S.G. Hess et al. “The Effectiveness of a School-Based Adolescent Depression Education Program.” Health Education & Behavior 37, no. 1 (2007): 11–22. https://doi.org/10.1177/1090198107303313.
Tkacz, J., and B.L. Brady. “Increasing Rate of Diagnosed Childhood Mental Illness in the United States: Incidence, Prevalence and Costs.” Public Health in Practice 2 (2021): 100204. https://doi.org/10.1016/j.puhip.2021.100204.
Thorton, E.M., and B. Miller. “Mental Health and Well-Being in Faith-Based Schools: A Qualitative Study.” In Leading Insights: Mental Health and Well-Being, edited by L. E. Swaner, 31–41. ACSI, 2022.
Townsend, L., R. Musci, E. Stuart et al. “The Association of School Climate, Depression Literacy, and Mental Health Stigma Among High School Students.” Journal of School Health 87, no. 8 (2017): 567–74. https://doi.org/10.1111/josh.12527.
US Census Bureau. National Survey of Children’s Health. USCB, 2023. https://www.census.gov/programs-surveys/nsch.html.
VanderWeele, T.J. “Religious Communities and Human Flourishing.” Current Directions in Psychological Science 26, no 5 (2017): 476–81. https://doi.org/10.1177/0963721417721526.
VanderWeele, T.J., B.R. Johnson, P.T. Bialowolski et al. “The Global Flourishing Study: Study Profile and Initial Results on Flourishing.” Nature Mental Health (2025). https://doi.org/10.1038/s44220-025-00423-5.
Wilson, A., E. Meier Thornton, K.L. Hauser, L. Miller, B. Volpone, and B.M. Miller. “Student Mental Health Support in Private Christian Schools: Perspectives and Needs.” Journal of Psychology and Christianity 42, no. 3 (2023): 187–207.